

Introduction
Malnutrition is one of the major problems of many developing countries associated with almost one-half of all child deaths globally.1 Today malnutrition not only affects individuals but its effects are passed from one generation to the next as malnourished mothers give birth to infants who struggle to develop and thrive; Survivors are left vulnerable to illnesses, stunted growth and intellectual impairment.2 About 30% of children (6 59 months) in the World-wide are stunted due to improper feeding and repeated infections.3 Optimal infant and young child-feeding (IYCF) practices such as exclusive breastfeeding for 180 days and nutritionally sufficient and safe weaning foods starting from 6 months are crucial for health and development, and lastly the survival of infants and young children.3,4 Introduction of solid, semi solid or soft foods after 6 months of birth can outweigh any potential risks and this is applicable for all countries irrespective of their socio-economic condition.5 Arifeen et al., (2001) reported in his previous study6 that infants who are not breastfed have 5 to 7 fold increased risks of death from diarrhea and pneumonia compared to exclusively breastfed infants aged 0-5 months.6 Good weaning practices at infancy are necessary for achieving and sustaining proper health, nutrition and development.7 Inappropriate feeding exercises, such as absence of breast feeding, premature or too late introduction of complementary and weaning foods, which is nutritionally insufficient, have negative effect for child growth and development particularly in developing countries.8
High prevalence of under nutrition and nutrition related problem exist in Bangladesh such as stunting, wasting, underweight, low birth weight, anemia, iodine deficiency disorders and Vitamin A deficiencies disorders etc.2 Although Saha et al., (2008)9 explored the influencing factors behind childhood malnutrition in Bangladesh,9 very few have addressed the determinants related to specific tribal groups. The Garo tribe is one such minority group, originally from Tibet,10 has very little data regarding the nutritional status of children and related feeding practice. This study was conducted to determine the nutritional status (stunting, wasting, and underweight) of young children, and the infant young children feeding practice among the selected Garo tribes. Similar data was also collected from nearby non-Garo households for comparison. Looking at infant and young children feeding practice among the mothers/care providers and prevalence of malnutrition, may help in designing future plans for activities in the different areas in regard to reduce malnutrition rate and promotion of infant’s young children feeding practices.
Methods and Materials
Place of Study
The study areas were the two different villages of Jolchotro and Jangalia at Madhupur Upazilla, Bangladesh.
Study Period
The study was conducted from September 2012 to December 2013.
Type of Study
A cross sectional study was adopted.
Study Population
This study was conducted among the selected infant and young children bearing mothers at Madhupur Upazilla in Tangail region, Bangladesh.
Sampling Technique and Sample Size
At the beginning of this study, a pilot survey was done in two different villages of Jolchotro (having 700 Garo population) and Jangalia (having 600 Garo population) at Madhupur under Tangail area, in Bangladesh. The study subject (child-mother pair) were selected purposively based on having infants (1-11 months) in the household. Data was collected regarding socio-economic conditions, anthropometry and food intake pattern etc. The minimum required sample-size was calculated using the formula: n=Z2pq/d2 where n=required sample-size, p=expected proportion, Z=95% confidence interval, and d=9% error. In Bangladesh, the proportion of child feeding (CF) practices among the mothers of 6-9 months old children is 74%.11 Therefore, p=74% was taken as the expected proportion, i.e. 0.74, and q is (1-p) = 0.26. A total number 180 mothers–child pair were selected by non-random convenience sampling method; half of them were Garo and another half were Non-Garo households from above two villages, with the same socioeconomic status. Data were collected by trained volunteers regarding IYCF perceptions and practices by interviewing the mothers using pre-designed, pre-tested, semi structured interviewer administered questionnaire.
Anthropometric Assessment
The anthropometric data were collected based on standard methods. Weight was recorded in kilogram and height was measured in to the nearest 0.1 cm.
Data Analysis
Z score were calculated from the WHO reference data set. Data are presented as frequency distribution using SPSS 14 windows program.
Results
A descriptive, cross sectional study was carried out from selected Garo and Non-Garo Households. The salient feature of this study was presented in the following sections:
Table 1: Monthly expenditure of Garo and Non-Garo household on foods
| Expenditure on foods (Tk.) | Garo n(%) | Non-Garo n(%) |
| <2,000 | 3 (3.33) | 14 (15.55) |
| 2,000-4,000 | 11 (12.22) | 35 (38.89) |
| 4,001-6,000 | 33 (36.66) | 25 (27.78) |
| 6,001-8,000 | 21 (23.33) | 11 (12.22) |
| 8,001-10,000 | 19 (21.11) | 5 (5.55) |
| 10,001-15,000 | 3 (3.33) | 0 (0.0) |
| 15,001-20,000 | 0 (00) | 0 (0.0) |
| Total | 90 (100) | 90 (100) |
In most of the Garo areas the maximum total expenditure on foods were Tk. 4001-6000 while in case of Non-Garo areas the maximum total cost was Tk. 2,000 to 4000 only. And only 3.33% Garo and 15.55% Non-Garo areas monthly expenditure on foods were <2000 taka (Table 1).
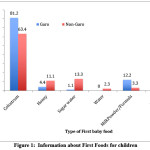 |
Figure 1: Information about First Foods for children Click here to View figure |
The above figure-1 shows the comparison of first feeding as a food in two groups where colostrum was given to their babies as a first food in Garo (81.2%) and Non Garo groups (63.4%) respectively. About 12.2% of Garo mothers first give powder\formula milk, while in Non-Garo area preference of giving more honey and sugar water are 11.1% and 13.3% respectively (Fig-1).
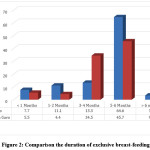 |
Figure 2: Comparison the duration of exclusive breast-feeding Click here to View figure |
Figure 2 shows the comparison the duration of exclusive breast feeding and indicates that 64.6% Garo and 45.7% Non-Garo mothers feed exclusively 5 to 6 times. On the other hand, 3 to 4 months both Garo and Non-Garo (13.3 and 34.5% respectively) did exclusive breast feeding.
Table 2: Comparison of the time of initiation of complementary foods to their babies
| Stage of complementary foods introduce | Garo N(%) | Non Garo N(%) |
| 1 month | 3 (3.33) | 0 (0.0) |
| 2 months | 9 (10) | 1(1.11) |
| 3 months | 7 (7.78) | 7 (7.78) |
| 4 months | 13 (14.44) | 33 (36.67) |
| 5 months | 22 (24.44) | 19 (21.11) |
| 6 months | 36(40) | 22 (24.44) |
| >6 months | 0 (0.0) | 8(8.89) |
| Total | 90 (100) | 90 (100) |
Table 2 shows the distribution of the all respondents about introduction of complementary foods to their babies and it is highlighted that 40% Garo mothers started complementary feeding at 6 months age of baby and 36.67% Non Garo mothers respectively started complementary feeding at 4 months age of baby.
Table 3: Name of first foods introduced as a complementary food
| First food introduced as complementary food | Garo n(%) | Non Garo n(%) |
| Milk /powder milk | 35(38.89) | 10(11.11) |
| Rice mashed | 0(0) | 20(22.22) |
| Suji | 22(24.44) | 14(15.55) |
| Vegetables | 6(6.66) | 4(4.44) |
| Fruit juice | 4(4.44) | 0(00) |
This table-3 indicates that about one third (38.39%) of the Garo infants and young children were given powder milk as first complementary food about half (46.67%) of the Non Garo infants and young children’s were given cow’s milk as first complementary food (Table-3).
Table 4: Frequency of complementary foods given per day
| Frequency per day | Garo n (%) | Non Garo n (%) |
| <4 | 35 (38.89) | 41 (45.55) |
| 5-6 | 27 (30) | 28 (31.11) |
| 7-8 | 20 (22.22) | 17 (18.89) |
| 9-10 | 8 (8.89) | 4 (4.44) |
| >10 | 0 (00) | 0 (0.0) |
| Total | 90 (100) | 90 (100) |
The table-4 indicates that majority of the infants in each group received complementary foods <4 times and 5-6 times per day mainly and this frequency depended on the infant’s age, mother’s available time and income of the family.
Table 5: Distribution of infants by the types of complementary foods within last 24 hours
| Food items | Garo | Non Garo | ||
| Frequency | Percent | Frequency | Percent | |
| Baby formula | 23 | 25.6 | 5 | 5.6 |
| Cow’s milk | 17 | 18.9 | 24 | 26.6 |
| Goat’s milk | 1 | 1.1 | 0 | 0 |
| A2nana | 7 | 7.7 | 5 | 5.6 |
| Green vegetables | 1 | 1.1 | 0 | 0 |
| Rice | 15 | 16.7 | 19 | 21.1 |
| Suzi (semolina) | 12 | 13.3 | 28 | 31.1 |
| Khichuri (Hotchpotch) | 14 | 15.6 | 8 | 8.9 |
| Fruit juice | 0 | 0.0 | 1 | 1.1 |
| Total | 90 | 100.0 | 100 | 100 |
Table-5 shows the type of complementary foods for the children of Garo and Non Garo mothers. It was found that 18.9% of Garo and 26.6% of Non Garo children received cow’s milk as complementary food. Other foods such as suzi (13.3%) for Garo and 31.1% for Non Garo, rice (16.7% for Garo and 21.1% for Non Garo) were used as complementary foods. About 25.6% Garo and 5.6% Non Garo used baby formula and only few percent used goat milk, banana, green vegetables, khichuri (Hotchpotch) and fruit juice.
Table 6: Mean, Standard Deviation of anthropometric indicators of infants
| Anthropometric Indicators | Garo (n= 90 ) | Non Garo ( n=90 ) | ||
| Mean | Standard deviation | Mean | Standard deviation | |
| Age (Month) | 5.12 | 0.87 | 5.71 | 0.76 |
| Length (cm) | 63.66 | 8.956 | 62.34 | 6.906 |
| Weight (Kg) | 6.63 | 2.224 | 6.70 | 2.071 |
| Height for age Z-score | -1.02 | 1.805 | -1.61 | 1.578 |
| Weight for age Z-score | -0.86 | 1.36 | -0.79 | 1.791 |
| Weight for height Z-score | -0.17 | 2.170 | 0.668 | 2.618 |
Table-6 shows the mean height and weight of the children (1-11 months) were 63.66 cm & 6.63 kg for Garo families and 62.34 cm & 6.70kg for Non Garo families. The Z score values for height for age and weight for height indicate that the infants from non-Garo households were more on the verge of stunting and wasting compared to their Garo counterparts.
Table 7: Nutritional status of the infants according to mid upper arm circumference (MUAC) classification
| MUAC (cm) | Classification | Garo n(%) | Non-Garo n(%) |
| <11.0 | Severe Acute Malnutrition | 0 | 0 |
| 11.0-12.49 | Moderate Acute Malnutrition | 9 (10) | 16 (17.78) |
| 12.5-13.5 | At risk of acute Malnutrition | 38 (42.22) | 44 (48.89) |
| >13.5 | Good Nutritional Status | 43 (47.78) | 30 (33.33) |
| Total | 90 (100) | 90 (100) |
According to mid upper arm circumference, a greater number of infants (17.78%) from non-Garo areas were moderately malnourished compared to infants in Garo areas (Table-7).
Discussion
Growth faltering and nutritional problems are common in infants and young children living in low- and middle-income countries. Although health and dietary intake are the immediate causes of malnutrition, child caring practices is another important component according to UNICEF model.12 Complementary feeding practices are essential component of infant feeding practices and are crucial for optimum infant and child nutrition.13
In the present study, most of the Garo and non-Garo children were malnourished and a lack of appropriate IYCF practice appeared to be responsible. The age for starting complementary feeding was 4 and 5 months for the majority of non-Garo participants, some of them delaying the process beyond 6 months of age. On the other hand, only 33% of the Garo mothers start complementary feeding after 6 months age of infants, which is in compliance with WHO recommendation.14 Previous studies had shown a significant association between untimely introduction of complementary foods and severe stunting and other forms of malnutrition.15 Studies have also showcased improvement in childhood nutritional status through appropriate initiation of weaning foods.16
Yet the extent of malnutrition for infants from non-Garo community was greater than those belonging to the Garo tribe. This finding is remarkable considering the Garo tribe is a marginalized and reclusive group. Introduction of colostrum was found to be higher among Garo respondents compared to non-Garo which justifies their greater prevalence of malnutrition. This is supported from evidence of previous studies such as by Kumar et al.,17 which had shown a positive relationship between deprivation of colostrum and stunting. Another study by Islam et al.,18 had obtained prevalence of stunting to be higher among children who had been deprived of colostrum, delayed introduction to breastfeeding and weaning foods.
Previous anthropological reports suggest the Garo tribe to have a strong matriarchal family system.19 Mother is the authoritative figure within the household and is the owner of whole family property, thus enjoying a high status.20 Needless to say, the decision-making power of mother translates to better feeding practice for infants. Recent literature shows that high maternal status or decision-making power might be one of the vital social factors in charge for influencing child’s nutritional health.21,22 Mothers are bound to utilize scarce resources for the benefit of their child if they are allowed to do as such.23 Our results show that Garo tribe have smaller families while the non-Garo families had a larger family size. But previous research have pointed out that it is not the household size but rather the total household income, expenditure on child rearing and maternal education that account for child nutritional status.24 Although both groups had been found to be living below the national average income, the Garo households consistently had higher spending on foods compared to non-Garo families. A very recent study on population level analysis of four countries that are India, Ethiopia, Peru and Vietnam showed a positive association between total household food expenditure and Height for age Z score.25 Mothers of Garo tribe also were more inclined to use appropriate baby formula instead of nutritionally inadequate cow’s milk or semolina as complementary food, compared to mothers of non-Garo community. Flawed complementary feeding practices intensified by nutritionally insufficient, and repeatedly contaminated, foods often introduced untimely remain a key cause of malnutrition.26
From the study we can conclude that a lot of deficiency in knowledge regarding optimum IYCF exists among the target groups. Future studies can be carried out to determine the extent to which the normative infant feeding practices, across all ethnic groups in Bangladesh, comply with international recommendations. This is necessitated since both groups of population investigated, Garo and non-Garo, had exhibited some form of malnutrition in spite of differing feeding practice. It will also be beneficial to examine the causative factors behind the lack of optimum infant feeding practices by choosing indicators that are culture and ethnicity sensitive for Bangladesh. Seeking inspiration from the Garo culture, it will also be essential to examine variables associated with maternal status (power over resources like food, income, knowledge, and esteem, within the family and in society at large) since mother is the primary caregiver and influence child’s growth. These can then be incorporated into many social programs that will promote optimum IYCF practice.
Conclusion and Recommendations
Majority of the Garo and non-Garo children are malnourished and a lack of appropriate IYCF practices appeared to be responsible. The study also concluded that Garo mothers had better IYCF practice compared to Non-Garo mothers which translated to lesser extent of stunting and wasting of children in the former group. Child nutrition should be deliberated as public health problem. An intervention needs to be developed to address the nutrition problem among underprivileged children in Bangladesh.
Acknowledgement
The author wishes to thank all the participants who were involved in this study. The author did not receive any financial assistance from any funding sources.
References
- WHO Child mortality. Who.int. https://www.who.int/pmnch/media/press_materials/fs/fs_mdg4_childmortality/en/. Published 2019. Accessed January 6, 2019
- Dewey K, Begum K. Long-term consequences of stunting in early life. Matern Child Nutr. 2011;7:5-18. doi:10.1111/j.1740-8709.2011.00349.x
CrossRef - Global Strategy for Infant and Young Child Feeding, WHO-UNICEF, 2003. who.int/nutrition/topics/global_strategy
- Ahmed T, Black RE, Cousens S, Dewey K, Giugliani E, et al., What works? Interventions for maternal and child under nutrition and survival. Lancet.2008;371:417–40.
CrossRef - Daelmans B, Martines J, Saadeh R. Conclusions of the Global Consultation on Complementary Feeding. Food Nutr Bull. 2003; 24(1):126-129. doi:10.1177/156482650302400107
CrossRef - Arifeen S, Black RE, Antelman G, Baqui A, Caulfield L, Becker S. Exclusive breastfeeding reduces acute respiratory infection and diarrhoea deaths among infants in Dhaka slums. Pediatrics. 2001;108:E 67.
CrossRef - Brown KH, Creed-Kanashiro H, Dewey KG. Optimal complementary feeding practices to prevent childhood malnutrition in developing countries. Food Nutr Bull 1995;16:164e.
CrossRef - Mamiro PS, Kolesteren P, Roberfroid D, Tatala S, Opsomer AS, Van Camp JH. Feeding practices and factors contributing to wasting, stunting, and iron-deficiency anaemia among 3–23-month old children in Kilosa District, rural Tanzania. J Health Popul Nutr 2005;23:222–30.
- Saha K, Frongillo E, Alam D, Arifeen S, Persson L, Rasmussen K. Appropriate infant feeding practices result in better growth of infants and young children in rural Bangladesh. Am J Clin Nutr. 2008;87(6):1852-1859. doi:10.1093/ajcn/87.6.1852
CrossRef - Jengcham S. Bangladesher Garo Samproday (The Garo community of Bangladesh), Dhaka, Bangladesh: Bangla Academy;1998.
- United Nations Children’s Fund. The state of the world’s children 2011. New York, NY: United Nations Children’s Fund, 2010. 52 p.
- The State of The World’s Children 2008. New York: UUICEF; 2008.
- Butte N, Wong W, Hopkinson J, Smith E, Ellis K. Infant Feeding Mode Affects Early Growth and Body Composition. Pediatrics. 2000;106(6):1355-1366. doi:10.1542/peds.106.6.1355
CrossRef - Infant And Young Child Feeding. Geneva: World Health Organization; 2009.
- Sethi R, Padhy S, Raju D. Knowledge, attitude and practices regarding complementary feeding among mothers of children 6 to 24 months of age in Konaseema region. Int J Contemp Pediatrics. 2017;4(2):394. doi:10.18203/2349-3291.ijcp20170451
CrossRef - National Health and Medical Research Council Infant Feeding Guidelines for Health Workers, 2003. New South Wales Public Health Bulletin. 2005;16(4):41. doi:10.1071/nb05010
CrossRef - Kumar D, Goel N, Mittal P, Misra P. Influence of infant-feeding practices on nutritional status of under-five children. The Indian Journal of Pediatrics. 2006;73(5):417-421. doi:10.1007/bf02758565
CrossRef - Islam, S., Mahanta, T., Sarma, R. and Hiranya, S. (2014). Nutritional status of under 5 children belonging to tribal population living in riverine (Char) areas of Dibrugarh district, Assam. Indian Journal of Community Medicine, 39(3), p.169.
CrossRef - Jengcham S. Bangladesher Garo Samproday (The Garo community of Bangladesh), Dhaka, Bangladesh: Bangla Academy;1998.
- Jalil M, Oakkas M. The family structure and cultural practices of Garo community in Bangladesh: An overview. Himalayan Journal of Sociology and Anthropology. 2012;5:95-110. doi:10.3126/hjsa.v5i0.7042
CrossRef - Brunson E, Shell-Duncan B, Steele M. Women’s autonomy and its relationship to children’s nutrition among the Rendille of northern Kenya. American Journal of Human Biology. 2009;21(1):55-64. doi:10.1002/ajhb.20815
CrossRef - Shroff M, Griffiths P, Adair L, Suchindran C, Bentley M. Maternal autonomy is inversely related to child stunting in Andhra Pradesh, India. Matern Child Nutr. 2009;5(1):64-74. doi:10.1111/j.1740-8709.2008.00161.x
CrossRef - Schmeer K. Married women’s resource position and household food expenditures in Cebu, Philippines. Journal of Marriage and Family. 2005;67(2):399-409. doi:10.1111/j.0022-2445.2005.00124.x
CrossRef - Iftikhar A, Bari A, Bano I, Masood Q. Impact of maternal education, employment and family size on nutritional status of children. Pak J Med Sci. 2017;33(6). doi:10.12669/pjms.336.13689
CrossRef - Humphries D, Dearden K, Crookston B, Woldehanna T, Penny M, Behrman J. Household food group expenditure patterns are associated with child anthropometry at ages 5, 8 and 12 years in Ethiopia, India, Peru and Vietnam. Economics & Human Biology. 2017;26:30-41. doi:10.1016/j.ehb.2017.02.001
CrossRef - Wielgosz A. FIFTY-NINTH WORLD HEALTH ASSEMBLY Agenda item 11.8. Infant and young child nutrition: quadrennial report Statement from the International Association for the Study of Obesity. Prevention and Control. 2005;1(4):330-331. doi:10.1016/j.precon.2006.06.003
CrossRef

This work is licensed under a Creative Commons Attribution 4.0 International License.






