
Introduction
Overweight and obesity
Overweight and obesity are a significant problem globally; the 2010 Global Burden of Disease Study announced that for the first time in history overeating was a more significant problem worldwide than starvation.1 A report published in April 2016 by NHS Digital found that 58% of women and 65% of men were either overweight (with a Body Mass Index [BMI] of between 25kg/m2 and 29.9kg/m2) or obese (≥30kg/m2),2 with obesity specifically increasing in prevalence from 15% of the population in 1993 to 26% in 2014.3 Unfortunately, in the UK alone the number of new obesity cases is predicted to reach up to 11 million per year by 2030, which could result in an additional financial burden of between £1.9 and 2 billion per year to cover the cost of treating what are considered to be preventable obesity-related diseases such as Type 2 diabetes, heart disease and certain types of cancer.4
Adherence
The WHO defines adherence as “the extent to which a person’s behaviour – taking medications, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a health care provider”.5
It appears to be influenced by multiple factors, with both patients and practitioners facing a wide range of barriers. The same report categorised these as social and economic factors, the care team and system, the characteristics of the disease, disease therapies and patient-related factors.5 In a literature review by Shay, 15 antecedents (events that must take place prior to the occurrence of the concept), were found to be associated with adherence (see Table 1 for summary).6 According to the World Health Organization (WHO), adherence is a major problem within healthcare, with up to 50% of patients suffering from chronic diseases after failing to adhere to a regimen of prescribed medications, diet and lifestyle interventions – resulting in poorer health outcomes and increased healthcare costs.5 According to Mintel (2014), despite up to 55% of the UK population dieting at some point during any given year, up to 19% claim they don’t have the “willpower to stick to the diet for very long”.7 Furthermore, adherence is found to be of greater significance to weight loss outcomes than the macronutrient content of a calorie-controlled diet (such as Atkins or the ‘Zone’ diet),8 an opinion shared by many dieters who appear to believe that “they all work… when you stick to them”.9 These findings strongly suggest that healthcare professionals working with individuals wishing to lose weight need to place greater emphasis on finding strategies to support client adherence, as opposed to focusing on the specific nutrient content of the diet.
Table 1: Antecedents to adherence summarised from Shay6
| Antecedent | Description |
| Self-efficacy | Found to increase adherence to physical activity and dietary adherence |
| Outcome | Lack of belief in intervention/medication reduces adherence |
| Perceived value | Belief that interventions (such as weight loss) are medically necessary increases adherence |
| Prior relapse | Number of times an individual has relapsed from a prior attempt reduces adherence |
| Time | Lack of time perceived to be a barrier to adherence to physical activity and nutrition advice |
| Environment | Lack of suitable place to exercise and availability of foods |
| Social support | Being in a couple increases adherence to physical activity and attending group sessions increases adherence to low-fats diets. Lack of social support contributes to poorer adherence to medications/therapies |
| Knowledge | Knowledge appears to be directly linked to adherence to medications, disease-management plans and diet |
| Socioeconomic status | Low socioeconomic status is associated with poor adherence to medications and diet; costs seen prohibitors |
| Perception of harm/adverse effect | Fear of harm and adverse events are associated with poor adherence to medications and physical activity |
| Active participation | Patient involvement enhances long-term dietary adherence |
| Provider influence | Open communication between patient and clinician, regarding treatment concerns, health goals and potential barriers increases adherence, whereas in contrast lack of available time and lack of interest on the part of the practitioner can have a negative impact on adherence |
| Mental health | Poor mental health found to reduce adherence |
| Motivation | Lack of motivation has a negative impact on adherence |
| Perceived goal attainability | Complicated medication regimens, dietary changes which are perceived to be excessive and higher intensity exercise programmes may have a negative impact on adherence |
For the purpose of this paper the term nutritional practitioner refers to nutritional therapists and dietitians. Individuals seeking support from a nutritional practitioner are referred to as clients.
Motivation for this research
There are currently a number of options available to individuals seeking support with weight loss, including support via their GP, working one-to-one with a nutritional practitioner such as a dietitian, nutritionist or nutritional therapist and joining some form of commercial weight loss club. Weight loss clubs have been shown to be twice as effective for weight loss than primary care programmes,10 however overweight and obese individuals may also seek personalised support for health concerns given the link between overweight and obesity and chronic health conditions.11 One of the benefits of a personalised approach is that the recommendations are tailored to the individual, however the benefits of group support cannot be provided in individual nutritional practice consultations.
A greater understanding of the factors which influence adherence to nutritional interventions, from the perspective of the client, is needed in order to inform nutritional practitioners so they can offer more effective weight loss solutions. As a first step, this study aims to identify some of these factors, from the experiences of individuals who have successfully lost weight whilst working with a nutritional practitioner.
Materials and methods
Research methodology
IPA was the chosen research methodology as it is concerned with “the detailed examination of the human lived experience”, which is consistent with the aims of this study.12
IPA has gained momentum within the field of Health Psychology, with research being conducted into areas such as illness experience, client and therapist experiences of therapy and eating disorders.13 It has also been employed in a growing number of weight management studies which have focused on the lived experiences of dieters from a number of different perspectives, including different demographics14 and weight loss success.15
IPA is considered to be a double heuristic approach, whereby the researcher is effectively interpreting the participant’s interpretation of a lived experience. One obvious limitation to this methodology is that it is entirely subjective, therefore reducing the likelihood that any two researchers would come to exactly the same conclusion. This can raise questions of validity, however, the inclusion of verbatim quotes within this paper aims to maintain the voice of the participants and provide the reader with greater understanding as to how the researcher arrived at the results. The researcher also reflexively considered positionality in order to understand her own potential for bias.
Both authors are nutritional therapists. During this study the researcher was training to be a nutritional therapist and therefore had “insider” knowledge of the process being examined in the study.16 This has likely to have impacted on the development of interview questions and interpretation of responses. Furthermore, the participants were aware of the researcher’s position and this may have had some influence on their answers; potentially encouraging them to speak more favourably about both the process and the practitioner as a result of social desirability:
“Social desirability is a research term that describes a type of response bias that is the tendency of survey respondents to answer questions in a manner that will be viewed favourably by others”.17
Conversely the researcher had only “outsider” knowledge of working with a nutritional practitioner for weight loss support, having never had experience of working with a nutrition practitioner for weight loss, which will have encouraged a greater degree of objectivity.
To conclude, whilst it is impossible to remove bias, its influence was considered prior to embarking on the research.
The methodological approach was designed in accordance with the guidelines set out by Smith in his book Interpretative Phenomenological Analysis, Theory, Method and Research18 and Pietkiewicz and Smith; A practical guide to using Interpretative Phenomenological Analysis in qualitative research psychology.19
Recruitment
Following approval from the CNELM Research Ethics Committee, in keeping with IPA requirements as laid out by Smith;18 four participants were recruited using purposive sampling, following the inclusion and exclusion criteria as set out in Table 2. Four participants were considered sufficient to enable in depth analysis within the time constraints, although data saturation may not have been achieved.
Table 2: Inclusion and exclusion criteria for study
| Inclusion Criteria | Exclusion Criteria |
| Participants must be adults (18 years and above). | Participants will not be minors (now or at the time they initiated diet and lifestyle changes to support weight loss). |
| Participants can be male or female. | Participants will not be suffering from a diagnosed mental disorder or be considered vulnerable. |
| Participants need to be English speaking (not required to be a first language, but good level of spoken English is highly preferable). | Participants will not be chosen when there is cause to think that weight loss may be or have been attributable to physical or emotional health issues (such as disease, eating disorders or stress), and thus not specifically intentional diet and lifestyle changes. |
| Participants will have sought advice from a nutritional practitioner for health issues including weight loss. | |
| Participants must have had a long-term history of weight management issues (not just seeking weight loss following a one-off event such as pregnancy or childbirth). For the purpose of this study, ‘long term’ will be defined as five years or more. This could either be a static weight, or fluctuating weight, as in the case of yo-yo dieting (or weight cycling). |
The participants
Three out of the four participants were recruited via a gatekeeper; these gatekeepers were nutritional practitioners who were contacted via email and invited to put forward clients. A fourth participant was recommended to the researcher via a mutual acquaintance.
Three of the participants had sought nutritional support from a nutritional therapist and one with a dietitian. Dietitians are a state regulated profession with a protected title, described by the British Dietetics Association (BDA) as:
“a degree-qualified health professional who: helps to promote nutritional well-being, treat disease and prevent nutrition-related problems, provides practical, safe advice, based on current scientific evidence and holds a graduate qualification in nutrition and dietetics in the UK” 20
Nutritional Therapist are positioned as complementary therapists who can choose to register voluntarily with both the Complementary and Natural Health Care Council (CNHC) which is accredited by the Professional Standards Agency (PSA) and the British Association of Applied Nutrition and Nutritional Therapy (BANT). The BANT definition of Nutritional Therapy is:
“Nutritional Therapy is the application of nutrition science in the promotion of health, peak performance and individual care… Practitioners consider each individual to be unique and recommend personalised nutrition and lifestyle programmes rather than a ‘one size fits all’ approach” 21
Whist there may be a number of differences between the method of practice between nutritional therapist and dietitians, and indeed between individual practitioners, this study focusses on individual client’s experiences of working with a nutritional practitioner and adhering to a weight loss intervention, not the practitioner’s individual approach.
Some demographic data were collected (see Table 3).
Table 3: Demographic data for participants
| P* | Name** | Gender | Region | Age | Reason for seeking support | Nutritional Practitioner |
| 1 | Alison | Female | South Lanarkshire | 54 | Menopause symptoms and weight loss | Privately funded nutritional therapist. Graduate of CNELM |
| 2 | Judy | Female | Buckinghamshire (originally from France) | 43 | Weight loss to help with conception | Dietitian – referred via NHS GP |
| 3 | Janet | Female | Avon | 59 | Weight loss and digestive issues | Privately funded nutritional therapist. Graduate of CNELM |
| 4 | Samir | Male | South Gloucestershire | 43 | Managing ankylosing spondylitis and weight loss | Privately funded nutritional therapist. Graduate of CNELM |
*P refers to participant number
**Names changed to protect identity
Participants 3 and 4 worked with the same nutritional therapist, which suggests their therapeutic experience was similar. Both nutritional therapists graduated from the Centre for Nutrition Education and Lifestyle Management (CNELM). CNELM’s Nutritional Therapy training includes health coaching so these practitioners have skills in motivating and helping clients to change health behaviour, which impacts client motivation and personal satisfaction.22 Collecting further demographic and socioeconomic data from the participants and practitioners may have enabled greater comparative analysis in order to identify their potential influence on adherence. None the less, all of the participants had achieved their own weight loss goals. This research aims to assess the participant’s views on weight loss adherence from their perspective.
Interview process
Three out of the four interviews were undertaken over online conference call, the fourth over the telephone due to last minute technical difficulties. The interviews were semi-structured, following the guidelines set out by Smith; a flexible interview schedule (see below), encouraging participants to talk freely and in depth about their experiences.23
Interview schedule
- What led you to see a nutritional practitioner?
- Can you tell me about your first appointment?
- What happened next – report, follow-up consultation, follow-up contact?
- How did you find following the programme/diet?
- How was this weight loss experience different from previous attempts?
- What motivated you to stick to the intervention?
- Is there anything else you would like to tell me about the process?
Each question was then expanded upon using predefined prompts such as ‘why was this helpful?’ and ‘how did this make you feel?’ to encourage participants to consider their experiences more fully.
Data analysis
Data analysis encompassed a series of steps based on the description set out by Smith (for an overview of the process, see Figure 1).24 At the end of the process a master list of superordinate and corresponding themes was used to produce a table of results which included verbatim examples of the themes from each of the four transcripts, where appropriate.
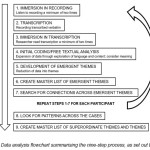 |
Figure 1: Data analysis flowchart summarising the nine-step process, as set out by Smith |
Transcription key
[…] indicates that text is missing
[laughs] italic text in square brackets indicates non-verbal communication or censored language e.g. laughter or expletives
[text] non-italic text in square brackets indicates implied but unspoken material
… indicates a pause
Results and Discussion
Overview of results
It is acknowledged that these themes only represent the accounts of four individuals who achieved weight loss whilst following a nutritional intervention and that these themes are subjective interpretations by the researcher. Verbatim extracts from the interviews will be included where appropriate to illustrate the themes and all names have been changed to protect identity.
These results are grouped into three superordinate themes; I trust this process, I feel valued, and understanding of self. Within these there are a further nine themes: (1) professional (what they do and what they know), (2) in-depth and thorough, (3) can’t argue with the results, (4) someone genuinely cares, (5) I am an important part of this process, (6) empowered by knowledge, (7) shift in focus towards health, (8) my motivation, and (9) this is who I am and what I need to do.
Superordinate theme – I trust this process
Trust suggests that there can be reliance on the integrity, strengths, ability and surety of a person or thing, which elicits confidence and hope. All four participants indicated they trusted or had faith in their nutritional practitioner, which encouraged both initial and ongoing adherence to the practitioners’ recommendations. This theme concurred with the findings from research into doctor-patient relationships, where trust was found to be strongly associated with confidence in doctors, and was a constituent part of “overall satisfaction”.25
Trust may also enable practitioners to have greater influence over their clients through “verbal persuasion”, where “individuals can be convinced of having the ability to do a behaviour through others telling them they are able to do it”.26
According to Bandura, author of Self-Efficacy: The Exercise of Control, verbal persuasion is one of four factors which influence self-efficacy, described as “the belief in one’s capabilities to organise and execute the courses of action required to produce given attainments.”27 Self-efficacy is thought to influence choice of behaviour, effort, length of persistence and emotional reaction in response to threat of failure, and is believed to play a significant role in adherence – both in terms of weight loss and maintenance. A clinical review undertaken by Cochrane looking into the strategies that could enable individuals to make healthier choices about their weight found that self-efficacy correlated positively to success in all realms of personal endeavour and helped overweight patients to become more self-reliant.28 There is also a strong correlation between self-efficacy and weight loss success.29, 30
‘I trust this process’ was made up of three themes: (1) professional (what they do and what they know), (2) in-depth and thorough, and (3) can’t argue with the results
Professional; what they do and what they know
According to a research report by the Health and Care Professions Council, professionalism is a “meta-skill, comprising of situational awareness and contextual judgement”. This is made up of a dynamic set of innate and learned skills such as knowledge, the ability to do one’s job, putting patients interests first and maintaining good standards of practice. Professionalism was also seen as a set of intrinsic qualities, such as empathy and caring and being moral and ethical. 31 All four participants in this study made either direct reference to their nutritional practitioner as a professional, or made comments pertaining to this:
I think [I took part] probably because it involved a professional and I wanted to follow it through to my best ability.
Well I guess it was sort of like a medical-type examination if you like […] so I was keen to try it to see if it worked.
Alison
Very easy. It’s not something I would discuss with anyone else. I don’t think any other health professional.
Janet
Having an expert at the end of the telephone is very good.
Alison
I could read all the books in the world and I would never know anything about it and you know enough about it and so therefore for me to go to a professional is the best route […] Because she had the knowledge. That is, that is the biggest point for me. So, I mean, therefore you could, you could trust.
Janet
A systematic review into the barriers which affect medication adherence reported a similar relationship, where a lack of confidence in physician professionalism had a negative impact on adherence.32
In-depth and thorough
This theme was most evident amongst the three participants who worked with a nutritional therapist. Participants described how their nutrition practitioner had looked into their cases very thoroughly, which appeared to give greater value to the subsequent recommendations:
She sent me a questionnaire which was quite lengthy and I filled it in to the best of my ability […] and it included all sorts of things like how I was feeling, how I was sleeping, what my toilet behaviour was […] It made me think about what a very detailed recommendation [it was]. I really felt that I needed to give it a go.
Alison
I think it just kind of focuses you on actually what you are doing and how, how you are feeling… So probably a good focus point.
Alison
I think I was asked about my symptoms first of all and what I wanted to achieve and then we went through various, actions and various things I could do and how I could divide, you know, between good fats and carbohydrates and protein […] Sarah then wrote up the report and she sent me the report. She listed everything we had discussed […] I didn’t expect it to be so thorough […] I didn’t expect her to go […] so deeply into the problems of my tummy and she did that as well, which really helped me.
Janet
Jane gave me a detailed report of our meeting. Her recommendations, where we were going to go forward and what’s going to happen in the next few weeks. […] Yeah, obviously because everything was itemised; what supplements I had to take when and where […]. She’d done a chart for me. Yeah it was really helpful and when one of them came to the end I would come and see her and she would re-evaluate what I needed.
Samir
This concept of “in-depth and thorough” was not identified through the background research, which may reflect the unique nature of a personalised nutritional approach. Nutritional therapy consultations tend to last between 60 and 90 minutes and involve taking an in-depth account of the client’s health history: including diet, medications and presenting symptoms. These are then considered in light of the client’s specific health-related goals (or reasons for seeking nutritional support) and any barriers to change. This process enables practitioners to develop highly personalised nutrition and lifestyle programmes for their clients.
Can’t argue with the results
Achieving results soon after implementing the interventions was a motivating factor. All four participants highlighted that achieving weight loss or a reduction in unwanted symptoms resulted in increased motivation to continue implementing nutritional changes. Recognising a connection between their actions (diet and lifestyle choices) and positive outcomes offered reassurance that what they were doing was working, and appeared to encourage continued adherence to their programme:
because it worked […] I lost weight so that was a good motivation.
Judy
The basic change I made was actually to get rid of gluten and wheat products […] And that just made such a difference […] When I could see that the weight was coming off, that was also an incentive to keep going […] And I think when you see something is working for you it’s much easier to keep it going […] And that if I didn’t stick to it, I had consequences […] And non-beneficial consequences. Painful ones.
Alison
I just took that out and I didn’t find any problems at all. And in fact, I felt considerably better after a week or so. […] [I stuck to it] because I felt better […] It made me feel better, a lot, lot better. I had more energy.
Janet
In contrast to the findings of this study, a lack of immediate improvement in symptoms may have a negative impact on adherence to medications.32
Interestingly, findings from research undertaken by Purcell (et al.) contradict the widely accepted guidelines that gradual weight loss is necessary for successful weight loss and maintenance in obese patients; in fact, the rate of weight loss was not found to affect the proportion of weight regained within the 144-week study period.33 Another study by Nackers (et al.) concurred with these findings; identifying both short and long-term advantages to fast initial weight loss, seeing greater overall weight reduction, long-term maintenance and no greater susceptibility to weight regain than gradual weight losers. 34 The authors also proposed that from a learning theory perspective “losing weight at a slow initial rate may be less reinforcing to participants than losing at a moderate or fast initial rate”.34
Such evidence of success, which in this study was seen as both weight loss and a reduction in symptoms, could also be classed as ‘Enactive Attainment’ or ‘Experience of Mastery’, which according to Bandura’s theory on self-efficacy, could increase self-efficacy.27 Self-efficacy was also a theme identified by Shay6 (see table 1). In short, if clients can discern that their nutritional programme is delivering results, it may encourage them to believe they have ‘mastered’ the ‘skill’ of losing weight, which in turn might increase self-efficacy and further encourage adherence (see Figure 2).
 |
Figure 2: Proposed link between evidence and adherence Click here to View figure |
One participant also found value in a different kind of evidence; results from a number of biochemical tests. Having results in “black and white” appeared to reinforce his resolve to adhere to dietary changes:
I mean gluten was discovered and I would never have had that tested if I hadn’t gone to see her […] so I would never have known […] So, I know now that every now and again when I have a little cheat, you know, that if I did cheat there’d be a reaction to it […] I mean could have guessed, but until you have it in black and white, which is what I had in black and white […] You know, it really, it really reinforces that you need to cut that out.
Even through if she’d told me, seeing it in black and white, you’re intolerant to that and that, yes you, you just can’t argue with it, can you?
Samir
Interestingly, a cross-sectional study into the impact of cancer diagnoses on the health behaviours of cancer survivors saw improvements in behaviours such as physical activity and diet one month after diagnosis, suggesting that a diagnosis may be a “cue to action”.35 Furthermore, disclosure of results from genetic tests for personalised nutrition appears to encourage greater adherence to nutritional programmes.36
Superordinate theme – I feel valued
This superordinate theme focused on the relationship between client and practitioner. Participants suggested they felt valued, respected and cared for by their nutrition practitioner. Two themes were identified within this superordinate theme: (4) someone genuinely cares, and (5) I am an important part of this process.
Someone genuinely cares
Elements of this theme were evident amongst all four participants. The nutritional practitioner was perceived to go above and beyond the job they were required to do and did so because they genuinely cared for their clients. Participants also perceived some form of emotional involvement on the part of the practitioner, which made clients feel both supported and valued:
More cared for […] People are doing that because they enjoy it […] She chose that. […] she cares for her patient, or hopefully for most of her patients, […] she enjoys teaching people to be healthier […] I suppose in some ways if someone cares enough for you to lose weight you feel well, not loved, but appreciated. […] You feel supported. You feel helped, someone is holding your hand. You know in a way […] It’s quite nice I suppose. It’s very individual […] And therefore it’s so much nicer because it’s targeted to you as well.
Judy
I felt she had my interests at heart.
Janet
It was really listening to what I was saying and then she would give me coping things targeted to me as opposed to… general[ised advice].
Judy
The practitioners’ commitment to their clients was also notable in their readiness and availability to help; their practitioner was always available, and nothing was too much trouble. This theme appeared to be stronger with the three clients who worked with a nutritional therapist, as opposed to the one client working with an NHS dietitian:
[…] I could contact her anytime, and say “I’m having problems with X Y and Z can you help? […] I know she’s there for me if I need her.
Alison
Yes, I mean I’m very lucky because I know I can always go back and ask.
Janet
All I gotta do is email, or text and she’ll get back to me if I’ve got a query […] I suppose [that’s] really reassuring, you know. Especially when I first started. I didn’t have a clue about gluten free stuff or [laughs] and er yeah, it’s really reassuring. If I sent her a text she’d actually answer back within the hour.
Samir
This level of ongoing support from the practitioners appeared to encourage commitment on the part of the client:
I felt I owed it to her and to me […] To be as strict as possible.
Alison
In relation to table 16, this theme could come under the heading “provider influence”. A review of the existing literature identified a desire amongst some dieters for ongoing support9 and that a lack of this has a negative impact on adherence to medications32. From a business perspective, practitioners are unlikely to be able to offer individuals unlimited support, but there do appear to be benefits to creating an environment where individuals feel they have access to ongoing support, both in the form of reviews, or opportunities to ‘touch base’ with their practitioner if they have questions or concerns.
I am an important part of this process
Participants described themselves as having an active role in the process; their input and feedback had value and they were working with their practitioner as part of a team. There was also a feeling that their practitioners were approachable and non-judgemental, creating a sense of mutual respect and accountability to one another:
We had a couple of chats after that and we made a few tweaks here and there […] There were some things that were working and some things that, that weren’t really, which we talked about them afterwards.
Alison
It was reassuring because I knew I could discuss all the supplements and what was going well. She could see if I was walking better as well. It gave her the reassurance that she was doing the right thing. It’s just I think, for her and for me to reassure each other that we were […] doing the right thing.
Samir
This relationship gave clients the confidence to speak out if they didn’t agree with a recommendation:
The only thing that I will say is she did say I.…should not have too much in the way of alcohol or caffeine. Caffeine was easier anyway, but I did say, ‘well I’m sorry but at the weekends I do have a drink!’ [laughs].
Alison
Participants also commented on an absence of guilt, or any sense that they were being judged if they weren’t managing to follow the interventions precisely. Two of the four participants described this as being an important and positive element of the relationship they had with their nutritional practitioner:
I think I was really relieved with the non-guilty feeling she allowed me to have. […] Which was nothing like I’ve had before like I found like in France […] Doctors, GPs tend to make you feel very guilty […] about your weight […] She was nice. She was never judgemental which was very nice.
Judy
I was never tempted to not take my supplements, but I was tempted to eat the wrong [laughs] thing occasionally. And when I did, you know, Sarah [would] just say ‘Tomorrow is another day […] This is today – we’ll be alright tomorrow.’ So, I found that fine.
Janet
The same two participants also made reference to the ease with which they felt able to open up to their practitioners, using phrases such as “easy to talk to”, “approachable” and “good rapport”:
I like the one-to-one rapport as opposed to being in a big room with one person talking and everybody else around you know saying you know I’ve lost that much and I’ve lost that much and if you haven’t you feel dreadful. And you know […] the rapport of the format of the session was nice.
Judy
I found Sarah very easy to talk to […] I think you’ve got to be totally honest and actually I thought I’d find that difficult because I knew Sarah outside […] I think Sarah is very approachable […] I’m not very good at discussing things about myself […] if Sarah hadn’t been so approachable I would have found that very difficult.
Janet
Whilst some dieters might work one-to-one with a GP, the relationship between client and nutritional practitioner may be different, due to the length and depth of the consultation, with nutritional therapy consultations tending to be 45 minutes or longer and Judy reported having a series of 30-minute sessions with her dietitian. A review by Martin and Downson into interpersonal relationships, motivation, engagement and achievement proposed that individuals have a tendency to take on and internalise the beliefs of significant others.37 The development of a positive relationship with clients may therefore enable practitioners to have greater influence over their client’s motivation and beliefs, including self-efficacy.
Participants in this study also recognised that they had entered into a partnership with their practitioner and were an active part of the process. In relation to table 16, this theme could come under the heading “active participation”. This notion of a partnership is recognised in the patient-centred approach to primary care,38 and is associated with lower levels of non-compliance to medications.39
Superordinate theme – Understanding of self
This superordinate theme included insights into how the participants thought about themselves; their motivations, values and beliefs. These were either inherent traits, or ones that had been developed during the weight loss process and are widely mirrored in the existing literature on weight loss. This superordinate theme was made up of four themes: (6) empowered by knowledge, (7) shift in focus towards health, (8) my motivation, and (9) this is who I am and what I need to do.
Empowered by knowledge
In relation to table 16, this theme could come under the heading “knowledge”. All four participants spoke of having a greater understanding of the ‘principals’ of healthy eating and had some understanding of the impact of food on their symptoms and overall health as a result of the work they did with their nutritional practitioner. This knowledge appeared to encourage commitment and gave them the understanding to make choices for themselves in the long term:
I can see the reasons why because I’d had it explained to me. […] I find it very difficult to do things if I don’t understand why I’m doing them.
Janet
Well she was basically just telling me to try and control my diet really. If I can control my diet […] it can have a link to the immune system […] to help the immune system really to fight the arthritis […] You know if I can help myself by my own, by eating the right foods, all the better, I think.
Samir
I still follow the general rules, I’m not a strict as I was. I was very, very strict in that first year or so […] I really did try and follow it to the letter almost […] a little less so now, but still the basic principles […] Basically, I feel if I stick to the guidelines which she has given me then I’m not going to go far wrong.
Alison
For me whatever she was teaching me was sustainable for my husband without me feeding him [expletive]. Ultimately when you have children, you know, you feed them good things as opposed to feeding them completely artificial, manmade products. So, for me it was more like in line with your life really.
Judy
This recognition for a need for knowledge and how this knowledge supported a successful weight loss outcome is clearly reflected within the existing literature, where knowledge was identified as a facilitator in weight loss40 and lack of knowledge, including confusion and conflicting information were attributed to diet failure.9, 41 Furthermore, the participants in this study understood that if they worked within certain guidelines, as opposed to a rigid set of rules, it was okay to deviate sometimes. This empowered them with a greater amount of choice and they felt less guilt when they deviated from the rules of their nutritional intervention. This shift in attitude away from a rigid set of rules and towards more relaxed guidelines may also help individuals to overcome dichotomous thinking (i.e. the ‘all or nothing’ approach), which is a common tendency amongst dieters, and has been attributed to diet failure. 40, 41
Shift in focus towards health
Three out of four participants identified improving their health as a central goal and did not appear to consider themselves as having been on a diet:
The end result was good, but it wasn’t the only thing […] End result was to lose weight, but the journey to it was to be healthy. […] More than the loss of weight in a way […] She [the dietitian] kind of like made me realise you have to go through a journey of being healthy, or healthier, as opposed to lose weight […] You know the weight loss is important obviously, but you know you can’t achieve long term weight loss without having the health with it.
Judy
I learnt from the start that I had to change. That it was a lifestyle thing, I think, as well, so I did start exercising more and stuff like that as well […] So, it brought to my mind a whole sort of healthy lifestyle […] It’s a lifestyle change […] And also, if you treat it like a kind of lifestyle thing, then it just becomes … it’s not like you’re punishing yourself, or being penalised in any way […] You’re not sort of rigidly sticking to something and if you do falter then you can you know, just pick up again which is… good.
Janet
Samir was very matter-of-fact about the changes he made and appeared to have readily accepted the fact that this was something he needed to commit to in the long term:
This is such as long-term thing now, over the last three or four years […] If you don’t stay on it, you can’t expect good results, can you?
In this study, irrespective of any initial weight loss goals, all participants appeared to hold the belief that overall health was more important than weight loss alone. This may have been an intrinsic belief in some cases or could have been developed as a result of working with the nutritional practitioner. Participants didn’t consider themselves to be on a diet; instead they saw their eating habits as a way of life.
In many instances diets are perceived to be a phase, where the approach to eating whilst on a diet differs largely to the approach either side of dieting,41 requiring a “state of heightened self-awareness and self-discipline with regard to eating behaviours” different from an individual’s natural state,42 potentially making diets more difficult to adhere to in the longer term.
My motivation
Motivation was also a theme identified by Shay6 (see table 1). When asked what motivated them to stick to the recommended interventions, all four participants described goals over and above just weight loss:
Trying to get some more energy levels and deal with some of the symptoms I was experiencing through that change of life […] I was desperate to try.
Alison
I had polycystic ovary syndrome […] It was difficult for me to have children and I knew that if I lost weight, it would help the whole process […] So, that was my ultimate goal.
Judy
I’d had some problems with my tummy and I put on a bit of weight and I was trying to lose weight a little bit, but I wasn’t getting anywhere […] But you want to sort it out because you want a better quality of life really.
Janet
Well I’ve got a form of arthritis called ankylosing spondylitis […] and I was just really struggling, and I was walking on crutches the whole time […] I thought, ‘I just can’t go on like this,’ (…) The main thing was to try and walk properly (…) When you’re hobbling around and you’re used to doing sport and being fit and you can’t walk properly it drags you down after a while, doesn’t it? […] I couldn’t do what I wanted to do really. It was also affecting my work. I was taking time off work.
Samir
Samir also identified the financial commitment he had made to the process as a strong factor. Having invested so much in the process, he felt he had to see it through:
[referring to spending a lot of money on tests] The money obviously [laughs] […] I spent a grand. If you spend a grand on tests and you think, well, you don’t want to waste that money, do you?
The existing literature concurred with the findings in this study, where motivation appears to be strongly associated with adherence. Webber (et al.) found that autonomous motivation (a measure of personal reasons for change, as opposed to perceived pressure from others to change), measured at four weeks, was a good predictor of longer term adherence to a 16-week weight loss programme, suggesting this may be a “promising intervention target for promoting program procedure adherence and weight loss”.43
Interestingly, the desire to lose weight for appearance-related reasons alone is actually associated with diet failure41, and this may be linked to a need for the benefits of change to justify the effort44. One example of this can be seen in a study by Gorin (et al.), who found that greater weight loss and lower weight regain after two years was seen in participants with medical triggers for weight loss, when compared to individuals with non-medical triggers.45 These findings suggest that if an individual has a significant amount of weight to lose they may need to be motivated by a more significant goal than weight loss alone.
This is who I am and what I need to do
This final theme saw participants demonstrating acceptance that they needed to follow a specific course of action to achieve their goals, that they recognised their personal weaknesses and how to navigate them, and a sense that they were taking responsibility for their own actions.
Alison, accepted she needed to remove gluten from her diet in order to support her health:
It’s a fact of life really. Yeah! ‘Here’s my bread roll! [laughs].
She was also conscious of her own limitations, acknowledging that if she deviated from the guidelines too much, she knew that she would go back to her old ways. This is something she has to pay attention to:
I don’t have to be totally strict … and its ok to deviate from time to time, but I think once you start deviating it’s very easy to fall back into the ways, for me anyway, so I just try not to.
Judy had accepted that she wasn’t prepared to go without unhealthy food completely, but believed she had developed a level of restraint which she didn’t have before working with the dietitian:
If I had a strong temptation, I think I didn’t overcome it [laughs]. I think I would give in, you know, [but] maybe with some restraint, thinking ‘okay let’s have one bar of chocolate […] and then have an apple or something,’ […] I don’t remember really giving in like, ‘I’m gonna eat three [bars of chocolate].’
She was also aware that giving up foods is challenging, but believed that it was just a process she had to go through:
I suppose you cut down and then you go through the hard days where you know you are still having your cravings […] time goes, as well, you have less cravings […] I think by then it was a whole kind of life.
Janet demonstrated that she understood how to navigate her temptation to deviate from her new diet without giving up altogether. She also believed that she had choices and was in control of the outcome:
I would just go and have it and then, you know, and then get rid of it and then just, you know, start again… it’s a choice you’re making. So, it feels like you have got lots of choice still.
Samir appeared to be quite black-and-white in his thinking. He described himself as living by the motto: ‘If you’re going to do it, do it properly’; he believed that if he had invested time, effort and money in something, it was worth doing. He also believed that his commitment was a crucial part of the process, without which his practitioner would not be able to help him:
Well, I mean, I think for me I spent nearly a grand to get my tests done and I was in a really bad way and I thought well what’s the point of it? Look! If you’re going to do it, do it properly. That’s my motto” […] You have to commit to doing it. You either want to do it or you don’t want to do it […] I think Jane was quite happy with that because she didn’t want to work with people who aren’t committed. You’ve got to be committed otherwise you’re wasting their time as well […] she can’t make a difference to people unless they’re committed.
Many of the themes in this study are associated with the participants’ beliefs: ideas that are accepted as true or real, or a firmly held opinion46. This included trust: in their nutritional practitioner and the recommendations (reinforced by successful weight loss or a reduction in symptoms); believing they were valued and an integral part of the weight-loss process; a belief in the importance of health versus only weight loss, belief in the value of their goals and feeling empowered to make choices for themselves. Some of these beliefs may have been innate, such as living by the motto, ‘if you’re going to do it, do it properly’, which may have always been this particular participant’s approach to life, whereas other beliefs may have been influenced by the process of working with a nutritional practitioner.
It is well documented that both motivation and self-efficacy 28, 29 are significant factors in weight loss, which is known to require significant and long-term behaviour changes to be successful. One method of supporting behavioural change is through health coaching; a goal-orientated process which often works at the level of motivation and belief. A review by Muñoz (et al.) which looked at the relationship between coaching and weight loss outcomes concluded that coaching was more effective at reducing anthropometric measurements associated with weight loss and at in increasing motivation, than education alone.22
Examples of the use of coaching for weight management or in the management of chronic disease include:
Motivational Interviewing (MI)
The purpose of MI is to help individuals overcome their ambivalence to change and can be described as “a collaborative conversation style for strengthening a person’s own motivation and commitment to change”.47
MI has been shown to increase retention to a weight loss trial, achieving 96% retention after 18 months; a significant increase on the 13–41% dropout rate seen in similar behavioural studies48 and supported both weight loss and glycaemic control in Type 2 diabetic women.49
The Transtheoretical Model (TTM)
TTM provides a “theoretical framework for approaches to accelerate the rate of behaviour change in a population”.50 TTM proposes that individuals have to pass through a series of five stages of change when transitioning from an unhealthy behaviour to a healthy one: precontemplation, contemplation, preparation, action and maintenance. TTM offers individuals stage-related strategies to support change. Considering weight management specifically, a transtheoretical model-based multiple behaviour intervention for weight management demonstrated significant improvements in healthy eating, exercise, managing emotional distress and weight loss.51
The 5As Behaviour-Change Model
This approach is promoted by The Person-Centred Care Resource Centre;52 practitioners aim to support change through a five-step process:
- Assess patient behaviour, beliefs and motivation.
- Advise the patient on risks and benefits of change (through education).
- Agree to a realistic set of goals.
- Assist with barriers to change.
- Arrange follow-up support.
Research into the effectiveness of the 5As approach in weight loss, found some correlation between weight loss success, and the number of ‘As’ utlilised by the physician; with ‘Assist’ and ‘Arrange’ being associated with diet improvement and ‘Advise’ being linked with increases in motivation and confidence to lose weight.53
Summary of Discussion
The results of this study, which are largely supported by findings in the existing literature, led the researcher to develop a proposed model for adherence to a nutritional intervention for weight loss (see Figure 3). This model identifies four main areas through which nutritional practitioners may be able to influence client adherence: professional practice, relationship with the client, coaching and education.
Professional practice
Clients appear to be motivated to follow the practitioner’s recommendations if they believe the practitioner to be professional, knowledgeable and thorough in their approach. This may be because the client’s perception of the value of the recommendations is then enhanced. Furthermore, if the nutritional intervention delivers results, both in terms of a reduction in symptoms and/or weight loss, this may encourage sustained adherence.
Relationship with client
Clients value a number of elements within the client/practitioner relationship: feeling genuinely cared for by their therapist, ongoing support/accessibility to their therapist, believing that they are an integral and valued part of the process, and that the therapist isn’t judging them.
Health Coaching
Practitioners may have the opportunity to influence client motivation and beliefs, such as self-efficacy, through various coaching strategies/behaviour change models – some of which show promising results in other weight loss studies.
Education
Practitioners have the opportunity educate their clients during consultations in order that they both understand the underlying rationale behind any nutritional (or lifestyle) recommendations and to empower them with the knowledge to make healthy choices for themselves in the longer term.
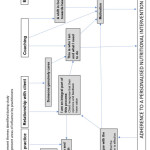 |
Figure 3: Adherence model Click here to View figure |
Conclusion and recommendations
The results of this study suggest that practitioners have a number of opportunities to support client adherence including many of the antecedents listed in table 16, and may benefit from incorporating the following into their nutritional practice in order to improve adherence:
- Maintain high levels of professionalism.
- Where appropriate, develop an intervention which delivers noticeable results in the short term (ensuring clients are aware of what to expect).
- Manage clients’ expectations, making them aware that they are an integral part of the process.
- Create an environment where clients feel able to contribute without feeling judged.
- Be accessible to clients and provide follow-up support.
- Educate clients so that they understand the rationale behind the intervention and give them the tools to make healthy choices for themselves.
- Consider incorporating coaching strategies alongside the intervention, to support behavioural change as part of a wider programme.
Whilst this study focused on adherence to weight loss interventions, the significance of the findings may not be limited to weight loss. Given that adherence is recognised as a problem within healthcare generally, future studies could be designed to include participants who worked with a nutritional practitioner and were required to adhere to a nutritional intervention for reasons other than weight loss. Research which identifies other influences on adherence to weight loss programmes, including demographic and social economic influences, may also be useful for nutritional practitioners in order to develop more effective weight loss solutions.
Acknowledgements
Thank you to all participants who made this research possible as well as the nutrition practitioners who connected us with their clients. With thanks to CNELM for providing research opportunities and support, in particular Kate Neil and James Neil for their feedback.
References
- Murray C. J. L., Vos T., Lozano R., Naghavi M., Flaxman A. D., Michaud C., et al. Disability-Adjusted Life Years (DALYS) For 291 Diseases and Injuries in 21 Regions, 1990–2010: A Systematic Analysis for the Global Burden of Disease Study 2010. Lancet: 380(9859): 2197–223: (2012).
CrossRef - [accessed 13 October 2017]. Available from: http://digital.nhs.uk/catalogue/PUB20562
- Lifestyle Statistics Team. Statistics on Obesity, Physical Activity and Diet. [accessed 7 April 2015]. Available from: http://www.hscic.gov.uk/catalogue/PUB16988/obes-phys-acti-diet-eng-2015.pdf
- Wang Y. C., McPherson K., Marsh T., Gortmaker S. L., Brown M. Health and Economic Burden of the Projected Obesity Trends in the USA and the UK. Lancet Elsevier; 378(9793): 815–25: (2011).
CrossRef - Adherence to long-term therapies: Evidence for action | World Health Organization. [accessed 12 November 2016]. Available from: http://www.who.int/chp/knowledge/publications/adherence_report/en/
- Shay L. E. A Concept Analysis: Adherence and Weight Loss. Nursing Forum: 43(1): 42–52: (2008).
CrossRef - Dieting in 2014? You’re not alone – 29 million Brits have tried to lose weight in the last year | Mintel.com. [accessed 3 July 2016]. Available from: http://www.mintel.com/press-centre/social-and-lifestyle/dieting-in-2014-you-are-not-alone
- Alhassan S., Kim S., Bersamin A., King A. C., Gardner C. D. Dietary Adherence and Weight Loss Success among Overweight Women: Results from the A to Z Weight Loss Study. International Journal of Obesity: 32(6): 985–91: (2008).
CrossRef - Thomas S. L., Hyde J., Karunaratne A., Kausman R., Komesaroff P. A. “They all Work…When You Stick to Them”: A Qualitative Investigation of Dieting, Weight Loss, and Physical Exercise, in Obese Individuals. Nutrition Journal: 7(1): 34: (2008).
CrossRef - Jebb S. A., Ahern A. L., Olson A. D., Aston L. M., Holzapfel C., Stoll J., et al. Primary Care Referral to a Commercial Provider for Weight Loss Treatment versus Standard Care: A Randomised Controlled Trial. Lancet: 378(9801):1485–92: (2011).
CrossRef - World Health Organization. [cited 13 October 2017]. Available from: http://www.who.int/topics/obesity/en/
- Smith J. A. The Theoretical Foundations of IPA. In: Smith J. A. (ed.) Interpretative Phenomenological Analysis Theory, Method and Analysis. London: SAGE Publications Ltd; 2009, 32.
CrossRef - Smith J. A. Evaluating the Contribution of Interpretative Phenomenological Analysis. Health Psychology Review: 5(1): 9–27: (2011).
- Mount A., Bogle V. The Dieting Experience: A Jewish Perspective. Journal of Health Psychology: 1(2006): 1–11. (2014).
- Alsawy S., Mansell W. How do People Achieve and Remain at a Comfortable Weight?: An Interpretative Phenomenological Analysis. Cognitive Behavioral Therapy: 6:ArtID E13: (2013).
- Greene, M. J. On the Inside Looking In: Methodological Insights and Challenges in Conducting Qualitative Insider Research. The Qualitative Report, 19(29), 1-13. (2014).
- Schoch AH, Raynor HA. Social desirability, not dietary restraint, is related to accuracy of reported dietary intake of a laboratory meal in females during a 24-hour recall. Eat Behav [Internet]. (2012).
CrossRef - Smith J. A. Planning an IPA Research Study. In: Smith J. A. (Ed.) Interpretative Phenomenological Analysis Theory, Method and Research. London: SAGE Publications Ltd; 2009.
- Pietkiewicz I., Smith J. A. A Practical Guide to Using Interpretative Phenomenological Analysis in Qualitative Research Psychology 1. Czas Psychologiczny: 18(2): 361–9: (2012).
- British Dietetic Association. What is a dietitian? Available from: https://www.bda.uk.com/foodfacts/WhatIsDietitian.pdf. 2014
- [Online]. Available from: http://bant.org.uk/about-nutritional-therapy/ [Accessed 17 December 2017].
- Muñoz Obino K. F., Aguiar Pereira C., Caron-Lienert R. S. Coaching and Barriers to Weight Loss: An Integrative Review. Diabetes, Metab Syndr Obes Targets Ther: 10:1–11: (2017).
- Smith J. A. Collecting data. In: Smith, J. A. (Ed.) Interpretative Phenomenological Analysis Theory, Method and Analysis. London: SAGE Publications Ltd; 2009.
- Smith J. A. Analysis. In: Smith J. A. (Ed.) Interpretative Phenomenological Analysis Theory, Method and Analysis. London: SAGE Publications Ltd; 2009.
- Van den Assem B., Dulewicz V. Doctors Trustworthiness, Practice Orientation, Performance and Patient Satisfaction. International Journal of Health Care Quality Assurance: 28(1): 82–95: (2013).
CrossRef - Lawrance L., Mcleroy K. R. Self-efficacy and Health Education. Journal of School Health: 56(8): 317–21 (1986).
CrossRef - Bandura A. Self-Efficacy: The Exercise of Control. New York: Freeman & Co Ltd; 1997.
- Cochrane G. Role for a Sense of Self-Worth in Weight-Loss Treatments: Helping Patients Develop Self-Efficacy. Canadian Family Physician: 54(4): 543–7: (2008).
- Edell B. H., Edington S., Herd B., O’Brien R. M., Witkin G. Self-Efficacy and Self-Motivation as Predictors of Weight Loss. Addictive Behavior: 12(1): 63–6: (1987).
CrossRef - Shin H., Shin J., Liu P. Y., Dutton G. R., Abood D. A., Ilich J. Z. Self-Efficacy Improves Weight Loss in Overweight/Obese Postmenopausal Women during a 6-Month Weight Loss Intervention. Nutrition Research: 31(11): 822–8: 2011.
CrossRef - HCPC-UKORGUK. [accessed 14 October 2017]. Available from: http://www.hcpc-uk.org.uk/assets/documents/10003771Professionalisminhealthcareprofessionals.pdf
- Yap A. F., Thirumoorthy T., Kwan Y. H. Systematic Review of the Barriers Affecting Medication Adherence in Older Adults. Geriatric Gerontology International: 1–9: (2015).
- Purcell K., Sumithran P., Prendergast L. A., Bouniu C. J., Delbridge E., Proietto J. The Effect of Rate of Weight Loss on Long-Term Weight Management: A Randomised Controlled Trial. Lancet Diabetes Endocrinol: 2(12): 954–62. (2013).
CrossRef - Nackers L. M., Ross K. M., Perri M. G. The Association between Rate of Initial Weight Loss and Long-Term Success in Obesity Treatment: Does Slow and Steady Win the Race? International Journal of Behavioral Medicine: 17(3): 161–7: (2010).
CrossRef - Humpel N., Magee C., Jones S. C. The Impact of a Cancer Diagnosis on the Health Behaviors of Cancer Survivors and their Family and Friends. Support Care Cancer. 15(6): 621–30: (2007).
- Nielsen D. E., El-Sohemy A. Disclosure of Genetic Information and Change in Dietary Intake: A Randomized Controlled Trial. DeAngelis M. M., (Ed.). PLoS One [Internet]. Public Library of Science; 9(11): e112665 (2014).
- Martin A. J., Dowson M. Interpersonal Relationships, Motivation, Engagement, and Achievement: Yields for Theory, Current Issues, and Educational Practice. Review of Educational Research: 79(1): 327–65: (2009).
- Little P., Everitt H., Williamson I., Warner G., Moore M., Gould C. et al. Preferences of Patients for Patient Centred Approach to Consultation in Primary Care: Observational Study. British Medical Journal: 322(7284): 468–72: (2001).
- Webb D. G., Horne R., Pinching A. J. Treatment-Related Empowerment: Preliminary Evaluation of a New Measure in Patients with Advanced HIV Disease. International Journal of STD and AIDS: 12(2):103–7: (2001).
- Rogerson D., Soltani H., Copeland R. The Weight-Loss Experience: A Qualitative Exploration. BioMed Central: 16(1): 371: (2016).
- Buchanan K., Sheffield J. Why Do Diets Fail?: An Exploration of Dieters Experiences Using Thematic Analysis. Journal of Health Psychology: 22(7):906–15: (2015).
- Green A. R., Larkin M., Sullivan V. Oh Stuff It! The Experience and Explanation of Diet Failure: An Exploration Using Interpretative Phenomenological Analysis. Journal of Health Psychology: 14(7): 997–1008: (2009).
- Webber K. H., Tate D. F., Ward D. S., Bowling J. M. Motivation and Its Relationship to Adherence to Self-monitoring and Weight Loss in a 16-week Internet Behavioral Weight Loss Intervention. Journal of Nutrition Education Behavior: 42(3): 161–7: (2010).
- Byrne S. M. Psychological aspects of weight maintenance and relapse in obesity. Journal of Psychosomatic Research: 53(5): 1029–36 (2002).
- Gorin A. A., Phelan S., Hill J. O., Wing R. R. Medical Triggers are Associated with Better Short- and Long-Term Weight Loss Outcomes. Preventative Medicine: 39(3): 612–6: (2004).
CrossRef - com. 1. Oxford Dictionaries | English. [accessed 15 October 2017]. Available from: https://en.oxforddictionaries.com/definition/belief
- Miller W., Rollnick S. Motivational Interviewing Helping People Change. New York: The Guildford Press; 2013.
- Goldberg J. H., Kiernan M. Innovative Techniques to Address Retention in a Behavioral Weight-Loss Trial. Health Education Research: 20(4): 439–47 (2005).
CrossRef - West D. S., Gore S. A., DiLillo V., Greene P. G., Bursac Z. Motivational Interviewing Improves Weight Loss in Women with Type 2 Diabetes. Diabetes Care: 30(5): 1081–7: (2007).
CrossRef - Greene G. W., Rossi S. R., Rossi J. S., Velicer W. F., Fava J. L., Prochaska J. O. Dietary Applications of the Stages of Change Model. Journal of the American Diet Association: 99(6): 673–8: (1999).
CrossRef - Johnson S. S., Paiva A. L., Cummins C. O., Johnson J. L., Dyment S. J., Wright J. A., et al. Transtheoretical Model-Based Multiple Behavior Intervention for Weight Management: Effectiveness on a Population Basis. Preventative Medicine: 46(3): 238–46: (2008).
CrossRef - [accessed 16 October 2017]. Available from: http://personcentredcare.health.org.uk/resources/5-behaviour-change-model
- Alexander S. C., Cox M. E., Boling Turer C. L., Lyna P., Østbye T., Tulsky J. A., et al. Do the Five A’s Work when Physicians Counsel about Weight Loss? Family Medicine 43(3): 179–84 (2011).

This work is licensed under a Creative Commons Attribution 4.0 International License.







