Introduction
Sodium consumption in India and its impact on health
Sodium, an essential nutrient, is tightly regulated by the human body. However when consumed in excessive amounts it has adverse cardiovascular and non cardiovascular health effects. The Osmotic properties of sodium make it determinant of extra cellular fluid (ECF) volume, including plasma and interstitial volumes. There for total body sodium determines blood volume and thus blood pressure (Meneton et al., 2005). The evidence points to a causal link between a chronically high salt intake and the development of hypertension when kidneys have a reduced ability to excrete salt (Meneton et al., 2005). While sodium is an essential nutrient in man, physiological need in acclimatized adults is only of the order of 8-10 mmol/day i.e.184-230 mg/day (Elliott and Brown, 2007) but in contrast, most adult populations around the world have higher average daily salt intakes. Different studies have already shown that too much sodium, mainly in the form of salt (sodium chloride), has adverse implication for health. Not only hypertension, salt may also cause renal and cardiovascular injury even in non-hypertensive population. Hypertension is responsible for 57 percent of all stroke deaths and 24 percent of all coronary heart disease death in India (Rodgers et al., 2000). A total of 1.2 million deaths were due to coronary heart disease and 0.5 million due to stroke (Murray and Lopez, 1997). It has been predicted that by 2020, there would be a 111% increase in cardiovascular deaths in India. The number of hypertensive individuals is anticipated to nearly double from 118 million in 2000 to 213 million by 2025 (Gupta, 2004). It is estimated that 16 per cent of ischaemic heart disease, 21 per cent of peripheral vascular disease, 24 per cent of acute myocardial infarctions and 29 per cent of strokes are attributable to hypertension underlining the huge impact effective hypertension prevention and control can have on reducing the rising burden of cardiovascular disease (Lim et al., 2012).
Salt in the form of sodium chloride is added to food mostly as table salt which is the major source of sodium in Indian diets. As per our social practices, diets rich in salt are consumed very frequently owing to large number of social or cultural events and even day to day life. With the increasing urbanization, consumption of fast food and eating outside has also increased among the people of the nation and is a trend that is agitatedly on with the present generation. Processed food is the dominant source for salt, unrestricted and uninformed use also contributes to the higher salt in India. The rising trend in the consumption of processed food in India has led to a 24-30% prevalence of hypertension in urban areas, and 12-14% in rural areas (Indus Health Plus, 2013). India has one of the largest snack markets of the world and people consume more than 400,000 tonnes of snacks every year (Sadasivam, 2004). Reasons why hypertension and heart disease have increased so dramatically in recent years are numerous and significantly include lifestyle, the amount of food eaten as well as changes in food consumption habits leading to high sodium consumption. Indian’s love of salt, consumption of more western along with traditional foods has continued unabated in present also, putting people at risk for high blood pressure, the leading cause of heart diseases. The recent global burden of disease study reports excess salt intake to be the 7th leading cause of mortality in South East Asia Region which is much higher than in rest of the world (11th globally), highlighting the adverse impact of high intake in countries like India (Lim et al.., 2012). In addition to raising the blood pressure dietary salt is responsible for several more harmful effects. A high salt intake increases the mass of the left ventricle, thickens and narrows resistance arteries, including the coronary and renal arteries. It also increases the number of strokes, the severity of cardiac failure and tendency for platelets to aggregate (Wardener and MacGregor, 2002). Saxena et al., (2011) conducted a study to estimate the prevalence of hypertension and to identify their biosocial correlates. A clinic based study was conducted in Rural Health Training Centre, District Garhwal of Uttraakhand on 1250 rural inhabitants. On the basis of salt intake the prevalence of hypertension was found to be 21.96% in the subjects consuming salt more than 8 gm/day. Salt intake was found to be a risk factor to cause hypertension. Apart from its effect on the cardiovascular system dietary salt has an effect on calcium and bone metabolism, which underlies the finding that in post- menopausal women salt intake controls bone density of the upper femur and pelvis. In renal disease, a high salt intake accelerates the rate of renal functional deterioration (Wardener and MacGregor, 2002). Of all the factors that relate to cancer of the stomach, the second most common cancer in the world, the relationship to salt is the strongest. Carcinoma of the stomach is strongly related to dietary sodium intake. There is some evidence which suggests that salt is associated with the severity of the asthma in male asthmatic subjects (Wardener and MacGregor, 2002).
Apart from health implications it has huge societal, developmental and economic costs. There is also noteworthy income loss to families affected by hypertension not only due to illness but also due to care giving and premature death (Mohan et al, 2013). Lifestyle diseases are expected to cost the Indian economy USD 6 trillion, in output losses between 2012 and 2035. This figure is nearly nine times India’s total health expenditure of USD 710 billion from 1993 to 2011 (Mukherjee et al., 2013). While these diseases are typically associated with the higher income classes and the urban demographic, India is seeing increasing penetration in rural areas as well with a rapid increase in sodium in the diet and this excess sodium intake can be a major driver of higher risk to cardiovascular diseases. Reducing salt intake has never been more relevant than it is today (Dobe, 2013). It is time for us to highlight the right approach to remain healthy in an environment of excess salt intake prevailing amongst the current generation of Indians and to close ranks against the growing threat of hypertension in India (Kalra et al., 2013). However, there is very limited contemporary data on population salt intake in developing countries like India. Some of the challenges for salt intake assessment include: high costs of measuring, limited national health surveys, paucity of food tables and food composition databases, lack of measure for added salt, lack of suitable tracking and accountability for local/ethnic foods, restaurants foods and foods from street vendors.
Meals eaten outside the home typically contribute to more sodium along with calories and fat. No guidelines for nutrition labeling exist for foods served in restaurant. Though fast food is certainly an occasional fun treat, many people tend to have it too often. Along with these, all Indian social and cultural events are associated with treats and sometimes results in unhealthy consumption of food which more prone to stage for irreversible health disasters for many. At these levels, the nutritious foods that an individual need for health, maintenance and optimal performance are being replaced by high sodium foods. Different chutneys, savoury sauces, pickle, tomato ketchups are some of the food items that are found to be frequently accomplished with the main meal and adds fair amount of sodium. Use of ready to eat foods (RTE) is also increasing in India which is found to have sodium content ranging from 480-6709 mg/100 gm (table1). Spices and condiments also adds fair amount of sodium (401- 10640 mg/ 100 gm) in Indian cuisines (table 1). The data given in table 1 has been compiled by the authors based on the nutritional information given on the package of the food products. Bread and grain products including pizza, pasta, noodles, breakfast cereals like cornflakes, provita, popcorn, roti /samosa/ spring rolls etc, which are consumed by the modern population very frequently, are found to be having sodium content ranging from 165-1940 mg/100g (Charlton et al., 2007). The situation in India is approaching critical levels. Figures showed that India consumes 55-58 lacs tons of edible salt annually and can reduce incidence of stroke by 25% and heart attacks by 10% by cutting down on salt consumption (Dobe, 2013). The urban Indian’s diet, pickled with takeaways and fast-food joints and instant foods that are ready in a jiffy and of course restaurant foods could worsen the present epidemic of hypertension due to its high proportion of salt. Foods that you would never think of, such as breads and many breakfast cereals, which the people prefer most to have in their busy life, are found to be very high in salt content. Johnson et al., (2012) undertook a study on Nutritional analysis of Junk Food. A total of 23 junk food samples from seven different food categories were collected from Delhi Outlets and analyzed for Salt, Total carbohydrates, Total Fat and Trans Fat content. One sample of potato chips was tested just for Total Fat and Trans fat content. The range of food categories tested in the survey included potato chips (4), Indian snacks (2), Instant noodles (2), Burgers (6), Pizzas (3), French Fries (2) and carbonated drinks (2) samples with a widely and internationally used methodology of Association of Official Analytical Chemists (AOAC). Each sample was analyzed in duplicate. Salt Content in the 22 junk food samples in g per 100 g of sample was in the range 0.2 to 4.2. The highest salt content was found in Instant noodles; Maggi Masala 4.2 g and Top ramen Noodles 3.2 g. Salt content in Potato Chips was 1.2-3.5 g per 100 g. Average salt content in vegetarian burgers (3) was 1.7 g and in non-vegetarian burgers (3) 1.5 g per 100 g. Average salt content in Pizza (3) was 1.0 g; in fries (3) 0.4 g and fried chicken (1) was 0.9 g per 100 g. Consumption of a packet of instant noodles, therefore, will cover about half of the daily salt quota. Salt content was not given by companies on the label. There should an all India action plan to reduce salt in diets and junk food companies should be asked to label salt quantity of their package. Even though research on salt consumption in population and various health issues is limited in Indian scenario, some existing studies indicates the high salt intake across different regions of India. Recently, ICMR- INDIAB Study also reported the average intake of 7.6 gm of salt among 124,000 individuals, covering all 28 states, the National Capital Territory of Delhi, and two of the union territories in the mainland of India (Times of India, 2014). Choudhary (2013) reported the average salt consumption of 42.3 gm/ day/ person in 1429 subjects residing in rural Andhra Pradesh by using household salt weighing method in year 2010. Radhika et al (2007) in their study conducted in Chennai city on 1902 subjects reported the significantly higher prevalence of hyper tension in subjects with highest quintile of salt intake. The mean dietary salt intake in the population found to be 8.5 g/d which was higher than the value recommended by World Health Organization. i.e. 5 g/d. A study was conducted by Jan et al (2006) on one hundred thirty five hypertensives and same number of normotensive residing in Kashmir and the mean levels of sodium excretion were found to be ranging from 424±150.50 mmol/L in hypertensive and 337±121.50 mmol/L in normotensive. A cross-sectional study was carried out by Ghosh et al (2013) in the field practice area of the Department of Community Medicine of tertiary care teaching institute of Bihar among adult population to find out the prevalence of hypertension and found a significant linear trend between age and salt intake with prevalence of hypertension. Although most information apart from the aforementioned study are not contemporary, these data indicate a high level of intake compared to the WHO recommended intake level of 5 g/day and the National Institute of Nutrition’s (NIN) recent Recommended Dietary Allowances (RDA) for Indians of 5–6 g/day (Mohan and Prabhakaran, 2013), which recommend salt reduction. But concerted action is still lacking to implement the guidelines nationally.
Reducing sodium consumption represents an urgent public health need in present scenario and is considered as an important and cost-effective measure for improving population health outcomes throughout the world and is promoted by WHO as a “Best Buy” or a cost-effective intervention even in resource limited settings (WHO, 2012). A population-wide reduction in sodium intake could prevent a large population of cardiovascular events in both normotensive and hypertensive population. For example, a population-wide decrease of 2mmHg diastolic blood pressure would be estimated to lower the prevalence of hypertension by 17 percent, coronary artery disease by 6 percent and the risk of stroke by 15 percent with many of the benefits occurring among patients with normal blood pressure (Mohan et al, 2009). He et al (2014) in the UK carried out a comprehensive analysis of the UK salt reduction programme with a view to providing a step-by-step guide to developing and implementing a national salt reduction strategy that other countries can follow. Key components of the UK salt reduction programme identified included (1) setting up an action group with strong leadership and scientific credibility; (2) determining salt intake by measuring 24-h urinary sodium, identifying the sources of salt by dietary record; (3) setting a target for population salt intake and developing a salt reduction strategy; (4) setting progressively lower salt targets for different categories of food, with a clear time frame for the industry to achieve; (5) working with the industry to reformulate food with less salt; (6) engaging and recruiting of ministerial support and potential threat of regulation by the Department of Health (DH); (7) clear nutritional labeling; (8) consumer awareness campaign; and (9) monitoring progress by (a) frequent surveys and media publicity of salt content in food, including naming and shaming, (b) repeated 24-h urinary sodium at 3-5 year intervals. The findings of the review indicated that the salt reduction programme which started in 2003/2004 has effectively reduced population salt intake by gradual reformulation on a voluntary basis. Evidence for this included reductions in salt content of many processed food and a 15% reduction in 24-hour urinary sodium over 7 years (from 9.5 to 8.1gm/day) (He et al., 2014). A systematic review was undertaken by Webster et al (2014) to provide a comprehensive overview of national initiatives to encourage the food industry to reduce salt in foods with a view to identifying which programs are more likely to have an impact. Out of the 83 countries that were indentified with salt reduction strategies, 59 countries reported programs of work with industry to reduce salt in foods. It was indicated that 23 out of the 59 countries reported industry meetings and 38 had established voluntary and/or mandatory sodium content targets. Thirty five countries established voluntary targets; 22 had voluntary targets for multiple food products, 8 had voluntary targets just for bread, 4 countries had targets for bread and processed meats and 1 country had targets just for dehydrated soups and sauces. Nine countries had established mandatory sodium targets, all of which had a target for bread. Seventeen countries reported reductions in salt levels in foods-the majority in bread. The study reported that a majority of the reductions reported (68%) were based on chemical analysis of food, except for Austria, Italy and Malaysia which were based on industry self-report, and Australia, Canada and the UK where reductions were based on product surveys. Many countries including the United States, Canada and Australia are following the UK’s lead and setting their own targets. It was concluded that the major challenge now is to engage other countries with local modifications stating that a reduction in salt intake worldwide will result in major public health improvements and cost savings (Webster et al., 2014). To ensure improved nutritional outcomes, consumer awareness is also critical. Though consumption choices are ultimately in the hands of the consumer, government and industry can play a major role in communicating nutrition recommendations to the consumer.
Understanding Agricultural Value Chain (AVC) and what is going off beam in India
Here the role of food industry and value chain can be identified to comply with all applicable legislative and regulatory provisions aimed at sodium reduction in foods during production – whether these foods are destined for consumers, other food manufacturers or the restaurant and other food service sectors. To understand well about the value chain, firstly it should be cleared that what is agriculture and how it relates to value chain and of course how it can work in lowering the sodium content in processed and packed foods. An agriculture refers to the production of food and non-food items through farming or animal husbandry, agribusiness refers to commercial agriculture, usually farms specializing in non-subsistence food and non-food production, and related businesses that are directly involved in the value chain of agricultural products (UNCTAD, 2009). Specifically, agro-food is a subset of agribusiness that refers to industries involved in the production, processing and inspection of solely food products made from agricultural commodities. Government bodies mandate rules, either at the seller or buyer end of transactions such as food product standards, food sanitation regulations, pesticide registration laws, and provisions of commerce mandated by specific commodity markets. The entire range of activities required to bring a product from the initial input-supply stage, through various phases of production, to its final market destination is generally identified with the concept of value chain (UNIDO, 2009). On the other hand, value chain is the sequential set of primary and support activities that an enterprise performs to turn inputs into value-added outputs for its external customers and is characterised by a market-focused collaboration of a set of enterprises working together to produce, process and market products and services in an effective and efficient manner. (Srinivasan, 2012).
However, value chains can also be seen as a vehicle for sodium reduction in processed and packaged food products at industry level. Government and stakeholders should work together to reduce the amount of sodium in processed and packed foods. But this work will be partial without public awareness and education activities to assist individuals so they can make informed food choices, guidance to the food industry about ways to reduce sodium in processed foods, and research to learn more about sodium reduction in the areas of food science and health. In countries like India the food value chain aiming towards sodium reduction is still nascent with limited knowledge and technology. Important barriers for developing country producers in this respect are the lack of an enabling environment offering institutional and infrastructural support, availability of resources and efficient and effective coordination in value chains (CTAC, 2009). The utilities of sodium have made it a crucial ingredient for many processed foods. It not only sustains the “life” of the food but it also provides a more economical approach to most companies (CTAC, 2009). Sodium chloride (salt) can prevent the development of food-borne pathogens. Because food manufacturers and producers often want to prolong the shelf life of their products, the amount of sodium in many processed foods is increased to certain levels. Aside from their preservation properties, sodium also helps bind ingredients (CTAC, 2009). It enhances the colour of the food, improves taste and function as a stabilizer. There are also regional and geographical differences in processed and packaged foods and in the country. Because of nutritional transition, have dual sources of salt. The growing globalization and consumption of processed foods high in sodium, ready-made food purchased from food vendors and changing dietary patterns add to the burden of increased salt intake. Most of the processed foods contain higher amounts of salt/sodium than you may expect. Some sources of sodium that are identified during formulation of the product are:
- From sodium chloride (salt) added;
- Intrinsic sodium in the food;
- From other ingredients added that contains sodium (emulsifier, dough conditioner, chemical preservatives, etc.). This type is often mentioned as sodium that is “hidden” from consumer’s knowledge eg. Baking soda, sodium bicarbonate, monosodium glutamate, sodium benzoate, sodium saccharin and sodium nitrate etc (CTAC, 2009).
Different countries have different salt sources in food and therefore in part need different strategies to reduce dietary salt. But at last most of the national and international agencies have acknowledged the role of lifestyle and diet, particularly in terms of sodium. It is a Best Buy for all income countries giving quick value for investment. Salt reduction can save a lot of lives if implemented as a systematic and sustained campaign. This will be achieved through the combined approach of food industry and government by implementation of an education and public awareness campaign and by engaging food and meal producers and distributors to reformulate their products. Though these food products are claimed to be manufactured using the best technology under most hygienic standards by trained professionals, they generally tend to be nutrient-poor and high calories, fats, sugars and salt ‘selling’ diet-related diseases like the cardiovascular diseases, diabetes, osteoporosis, certain forms of cancer, and high blood pressure and of course obesity (He and McGregor,2009). Government have to encourage all the stakeholders to voluntarily include sodium reduction in their guidelines, policies and procedures. Without any involvement, food industry may likely to result in increased salt intake more so with nutrition transformation as multinational food companies are specifically targeting developing economies like India for growth.
Food processors and manufacturers often use pervasive marketing techniques to create consumer demand for high-salt foods, which undermine efforts of public health and individual education interventions that attempt to reduce sodium intake. Food business operators are still trying their level best to maximize product sales or service operations and leave the negative consequences of such food consumption to be the result of free choice of consumers. Some food stuffs like pastries, burgers, sweets, pizzas and carbonated soft drinks are not so harmful but are poor in nutritive value with rich fat, sugar and salts content acts like a slow poison causing obesity and other diseases. Because sodium is found in many foods that we eat daily, guiding benchmark sodium reduction levels have to be set for almost all processed food categories especially those that are getting consumed at daily basis and that contain added or intrinsic sodium. Manufacturers are asked to apply this guidance to all processed food products regardless of whether the foods are destined for consumers, other food manufacturers, or for the food service and restaurant sectors.
To conclude, it is not only in the hands of food companies or the Government or the interested groups at large to create a healthy society but a more patronage and sustaining effort is required from the consumers themselves to make the world a better place to lead a meaningful life. Before initiating any salt reduction efforts, a comprehensive baseline analysis of key country stakeholders to evaluate their current knowledge, attitudes, practices and receptiveness to a range of salt reduction policy intervention option should be undertaken. These can include government representatives, health care organizations, civil society organizations, industry, consumers and academia. As such the role of Government/Regulatory bodies and public interest groups to intervene and regulate marketing practices of food business operators especially branded players has become a serious issue for debate now a days. Though the ultimate motive behind any business is to sell more and earn good profits for the shareholders in a legal way, huge personal and societal costs are associated with unregulated consumption of junk food stuffs. This is evidenced by heavy health costs of various diseases caused due to the over consumption of such foods. These costs affect everyone as they lead to higher medical costs and taxes (Jayadevan, 2012).
Cutting off the salt at industrial level
Today, nearly all populations consume far greater quantities of salt than those provided in natural, unprocessed food diets. The World Health Organization currently recommends a daily consumption of less than 5 grams of salt. Although there is a general lack of awareness of salt as a health issue in the nation, some countries with established salt reduction programs show increasing awareness. Many countries have brought into force various regulations and restrictions with regard to the promotional activities of fast food marketers in order to reduce its usage and avoid the related ill effects on the society. Same efforts we are also expecting in India. In India, the NIN has recently released new RD As for Indians that recommend salt reduction. Following this, some research bodies has been initiated studies to gather evidence to facilitate national salt reduction policy development. A knowledge translational clustered trial (DISHA-Diet and Lifestyle Intervention S for Hypertension Risk reduction through Anganwadi workers and ASHA-Accredited Social Health Activists) that aims to utilize grassroots health workers in the community across selected states of India is currently underway to evaluate the feasibility and impact of structured health promotion strategies (including those focused on salt) on population blood pressure reduction (Mohan and Prabhakaran, 2013). The findings will definitely be targeted primarily at public health policymakers and advocates. A variety of strategies will likely be needed for the purpose, such as those that increase access to affordable healthful foods in the community or add to individual’s knowledge of healthier food choices and motivations to try them. Education and knowledge translation needs to be given to policy makers, health care professionals, and general public and the food industry. Guidelines for the food industry should be in place for reduction in sodium additives to foods (packaged, restaurant, street food, or even home cooking) during processing/preparation. The entire food value chain in India is controlled by multiple ministries, department and laws. Here, political pressure can also create impact to implement policies that allow for a healthy food supply which supplies optimum levels of salt and other nutrients for good health. Strict yet practical targets and timelines need to be set and adequately monitored and evaluated with defined or inferred consequences. A comprehensive policy can ensure various initiatives across the departments that are aligned to ensure food safety. It will provide action agendas for all stakeholders in food value chain from government, producers, supply chain, food processing companies and distribution to focus on prioritized areas. Sodium reduction is an important part of healthy living and government have to work towards supporting the sodium reduction efforts and to provide guidance to the food industry to safely lower the amount of sodium in processed foods. Figure 1 depict as an example how the potential elements of a food procurement policy may work to influence individual, social, environmental, and biological factors to reduce sodium consumption and produce improved health outcomes such as decreased blood pressure and associated morbidity and mortality (Centers for Disease Control and Prevention, 2011). A systematic effort to reformulate food products to reduce their salt content is therefore a promising strategy for lowering the nation’s population salt intake. Food procurement policies can target many nutrients and set standards for sodium, calories, fat, trans fat, and sugar to increase the overall healthfulness of food options and provide a more healthful food environment.
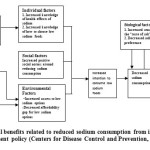 |
Figure 1: Potential benefits related to reduced sodium consumption from implementing a food procurement policy (Centers for Disease Control and Prevention, 2011). Click here to View figure |
Procurement policies can change the role of state and local government from a passive consumer to an active driver of the market, in the process providing greater demand for and access to healthful foods. The most effective way to reduce sodium would be for the agencies like Food Safety and Standards Authority of India (FSSAI) to set sodium limits for categories of processed foods that are the biggest sources of sodium. The limits could be based on the levels in the lowest-sodium brands, or on the given level of sodium content, in each category. Companies would be given several years to comply. Judging from the wide variation in sodium levels in competing brands of the same products, many companies could reduce levels significantly and easily. Once companies were in compliance, the limits could be reduced to the new level (or other lower) value but monitoring sodium content in the food supply is essential to evaluate the progress. The Central Government shall, by notification, establish a body to be known as the Food Safety and Standards Authority of India to exercise the powers conferred on under Food Safety and Standards Act specifically for sodium reduction in processed foods. Food industry should work to comply with all applicable legislative and regulatory provisions for the production, marketing and sale of foods. A concerted effort involving the individual, health care providers, governments, various organizations as well as the food processing industry can help to overcome the health hazards posed by excess salt consumption, as is being demonstrated in some of the nations. One another factor that can be contributed in salt reduction programme is food labeling, an important strategy to raise awareness and educate the public about salt. It has contributed to reduced salt consumption in many countries. Simple but effective consumer-friendly labeling indicating salt content in foods as currently in place in the UK can contribute significantly to salt reduction efforts. Government in collaboration with food sector should develop and mandatorily implement evidence-based but contextual labeling that will enable the population in choosing healthier foods (Mohan and Prabhakaran, 2013). The lay person does not consider salt as a threat to health and well being, because quantities in which it is consumed is seen as visibly less. Even they can’t recognise the difference between salt and sodium. Sometimes food companies mislead the public by giving the sodium content of the particular food item in grams rather than milligrams. Individuals are not aware about this unusual practice. A big and sustained task to done by food industries is to act honestly, responsibly and establish a strong nutrition policy. In many nations, food labels mentioning the content of sodium are mandatory. More recently, the UK has initiated a national salt reduction program based on collaboration with the food sector, implementing labeling using traffic light colours (Fig.2) and improving public awareness (Food Standard Agency, 2013).
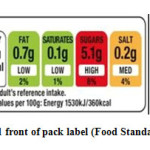 |
Figure 2: Proposed front of pack label (Food Standard Agency, 2013)Click here to View figure |
Finland launched a successful salt reduction campaign as part of a comprehensive strategy to lower the high incidence of cardiovascular disease in 1979. It was estimated that industry had formulated a variety of product groups which resulted in a reduced salt content of approximately 20% to 25%. This comprehensive approach has resulted in a one-third reduction in average sodium intake, from over 5000 mg per day in 1980 to about 3300 mg in 2002. This reduction contributed to a decrease of more than 10 mm Hg in the population average systolic and diastolic blood pressure, along with a 75% decrease in both stroke and coronary heart disease mortality and thus provides one of the best examples of a country achieving salt reduction through implementation of sound public health policies (Bureau of Nutritional sciences, Food Directorate, Health Products and Food Branch, Canada, 2012). Important factors that contributed to this decline in salt consumption included the adoption of a systematic approach with strong leadership, consumer education using mass media, regular monitoring of population salt intake through 24‐hour urine assessments and dietary surveys, intensive community and stakeholder engagement, cooperation with and oversight of the food industry, use of low sodium potassium‐enriched substitute (PANSALT®) and mandatory food labeling with high salt warnings (Mohan and Prabhakaran, 2013). Experience in these countries indicates that some of the key strategies for successfully reducing population salt intake are:
- Collaborative partnerships with the food sector along with regulation, particularly in the absence of voluntary action,
- Reformulating processed foods that are high in salt and account for a high percentage of intake,
- Implementing effective and context specific consumer education programmes on the effects of excess salt consumption on health,
- Implementing mandatory easy- to- understand and consumer –friendly food labeling to identify low salt products, as well as
- Creating an enabling environment to make healthy dietary choices easier by increasing the access to and availability of low salt as well as healthy foods (Mohan and Prabhakaran, 2013).
International bodies which regulate the media advertisements include confederation of food and drink industries of Europe (CIAA) and Union of European beverages association (UNESDA). It facilitates the development of an environment where all the European food and drink companies can meet the needs of consumers and society. It has laid down principles for food and beverage product advertisement. Union of European beverages association (UNESDA), in addition has laid down guidelines to restrict marketing communication to be placed in printed media, web sites, or programs (Jayadevan, 2012). Now the question arises that can it be worked in country like India where local street vendors are making the condition more alarming? People are fond of eating these local available street foods like kachori, samosa, pakoras, panipuries, aaloo tikki etc which get consumed with accompanied salty chutneys and sauces. Vendors are adding undefined salt in these products to make its taste accepted by the consumers and making them addicted to it. Mechanisms need to be in place to maintain transparency in engagement and to ensure that the food sector follows up on promised targets for reductions in salt and is independently monitored. Agriculture Value Chain can take a leadership role to continue to reduce sodium additives to foods during processing and preparation of all foods sold in the country and can also make readily available on overhead menu boards and table menus nutritional information, including the sodium content, for all foods sold in food service outlets. Marketing and advertisement of the salt reduction campaign can also contribute in creating awareness along with the value chain involvement. We have a long history of both sustainability and the use of marketing and market research to promote behaviour change e.g. use of iodized salt, washing your hands campaign etc. This time also we can succeed in tackling the big sustainability challenges regarding sodium reduction.
Table 1: Sodium content of different packed foods as given on the packages of the food products
|
S. No |
Food stuff |
|
Sodium content* (mg/100 g) |
|
1 |
Salt |
33200-38700 |
|
|
2 |
Baking powder (sodium bicarbonate) |
11420 |
|
|
3 |
Beverages (eg. Preserved fruit juices, squashes, energy drinks) |
222-22640 |
|
|
4 |
Preserved food pastes (eg.ginger, garlic pastes, tomato puries) |
775-10000 |
|
|
5 |
Ready to eat packaged foods (eg. Instant noodles, vegetables) |
480-6709 |
|
|
6 |
Soups |
3877-5378 |
|
|
7 |
Spices and condiments |
401-10640 |
|
|
8 |
Pickles |
4600-4900 |
|
|
9 |
Noodles |
1242-1932 |
|
|
10 |
Papads |
840-1745 |
|
|
11 |
Cheese and cheese spreads |
840-1442 |
|
|
12 |
Mixes for making foods (eg. Idli-dosa mix, dhokla mix, pakoda mix) |
580-1200 |
|
|
13 |
Sauces |
1070 |
|
|
14 |
Namkeens |
203-1060 |
|
|
15 |
Butter |
650-875 |
|
|
16 |
Processed breakfast cereals (eg. Corn flakes, wheat flakes, museli) |
400-770 |
|
|
17 |
Chips |
476-590 |
|
|
18 |
Breads and buns |
265-501 |
|
|
19 |
Biscuits and cookies |
167-430 |
|
|
20 |
Milk supplements |
400 |
Discussion
Salt is just there, right before you. Hence, it is for you to decide whether you want to eat it or not. Keep your eyes and decision-making mind charged up whenever you are going for grocery shopping. Many processed and convenience foods, preserved foods and sun-dried foods as well as canned foods contribute to higher intakes of salt. Check salt contents in cooking sauces such as soy sauce and ready-mix seasonings as some of these are very high in salt and finally eat more at home. Read labels on food to check salt contents. Be aware of nutrition issues and food composition with the aim of making more informed choices at the grocery store, while cooking at home, or when eating out and educate themselves and their families on healthy living practices, including healthy eating and adequate physical activity. Develop a taste for foods without salt or those that are low in salt. Sodium content in natural diets in general is itself very high. Cereals, pulses, vegetables, milk and animal and sea foods are the major sources of sodium. Restrict intake of preserved and processed foods like papads, pickles, sauces, salted biscuits, chips, nuts and cheese. Do not sprinkle just because it is there. Eat plenty of vegetables and fruits to get your intake of adequate potassium. The favourable part for Indians is that most food products in India, like fruits and vegetables and milk, have a wide availability across the country, which is very unique to India. This can leads to lower need for packaging and preserving food for transportation over longer distances and hence the addition of salt/sodium during processing and preservation. Consumers can use these tips when they cook at home, shop in the supermarket, or choose a meal at their favourite restaurant. Chefs and product developers can tap these ideas in the professional kitchen. Media representatives, healthcare professionals, and food marketers can mine this list for ways to promote positive and delicious nutrition messages about cutting salt. Voluntary cooperation between the government and the food industry to include appropriate labeling about the salt content on products and to ensure a stepwise reduction of salt in commonly consumed processed foods (Dobe, 2013). There is huge potential for major gains through sustained inter-sectoral action involving other concerned ministries and agencies. When consumers are offered a lower sodium product, they typically do not add table salt to compensate for the lower sodium content, even when available. Therefore, any program for reducing the salt consumption of a population should concentrate primarily on reducing the salt used during food processing and on changes in food selection (e.g., more fresh, less processed items, less sodium-dense foods) and preparation. In a rapidly changing society where processed and often salty fast food is served in canteens, worksite, restaurants and schools, new and reliable data on salt intake are therefore urgently needed. Indian government needs to develop programs and adopt regulations that would decrease the sodium content of the food supply, for the sake of the nation’s health. The Nutrition Facts Label on food and beverage packages is a useful tool for making healthful dietary choices and monitoring how much sodium is contained in a food you are considering. Consumers need to read labels carefully and choose lower-sodium products, for the sake of their own health. It is the time to close ranks against the growing threat of hypertension and cardiovascular diseases in India and the potential elements of a food procurement policy of national food agency may work to influence individual, social, environmental, and biological factors to reduce sodium consumption and produce improved health outcomes such as decreased blood pressure and associated morbidity and mortality. Yet some food manufacturers has already initiated sodium reduction in processed and packaged food products and some institutes and organizations are also supporting them in this health oriented task, but we need to be go so far to achieve the target of nation’s health. The active participation of food industries along with research organizations, NGO’s, media, public talks, reaching out public through education materials, school level nutrition education of children, awareness of medical doctors and also bringing in the information of Salt and Health even on labels perhaps realize people that they are unnecessarily taking more salt at the cost of their health. It may bring back a certain amount of caution in using salt which can in the long term contribute to a healthy society.
References
- Meneton P., Jeunemaitre X., de Wardener H.E., and MacGregor G.A. Physiol. Rev., 85, 679-715, (2005).
CrossRef - Elliott P. and Brown I. Background Document Prepared for Forum and Technical Meeting on Reducing Salt Intake in Populations, (2007).
- Rodgers A., Lawes C. and MacMohan S. J. Hypertens., 18, S3-S6, (2000).
CrossRef - Murray C.J.L. and Lopez A.D. The Lancet, 349, 1269-1276, (1997).
CrossRef - Gupta R. J. Hum. Hypertens.,18, 73-78, ( 2004).
CrossRef - Lim S.S., Vos T., Flaxman A.D., Danaei G., Shibuya K., Adair-Rohani H., Amann M., Anderson H.R., Andrews K.G., Aryee M., Atkinson C., Bacchu L., Bahalim A.N., Balakrishna K., Balmes J., Barker-Collo S., Baxter A., Bell M.L., Blore J.D., Blyth F., Bonner C., Borges G., Bourne R. et al. The Lancet, 380, 2224-2260, (2012).
CrossRef - Indus health plus. Salt consumption and prevention. Available at http://www.indushealthplus.com/salt-consumption-prevention/.
- Sadasivam V.S. Food and Nutrition paper. Food and Agriculture organization, Geneva, 215-30, (2004).
- Saxena P, Saxena V, Saxena Y. Ind. J. Comm. Health., 23, 81-83, (2011).
- Wardener H.E. and MacGregor G.A. J. Hum. Hyperten., 16, 213-223, (2002).
CrossRef - Mohan S., Campbell N. and Chocklingam A. Ind. J. Med. Res., 137, 627-631, (2013).
- Mukherjee D., Bajaj H., Garg N., Abraham J. FICCI survey on challenges in food processing sector, (2013).
- Dobe M. Ind. J. Pub. Healt., 57, 1-3, (2013).
- Kalra S., Sahay M. and Baruah M.P. J .Med .Nutr. and Nutraceut., 2, 1-2, (2013).
CrossRef - Charlton K.E., Steyn K., Levitt N.S., Jonathan D., Zulu J.V. and Nel J.H. Pub. Healt. Nutri., 11, 83-94, (2007).
- Johnson S., Sahu R. and Saxena P. Centre for Science and Environment, (2012) Available from: Website: www.cseindia.org
- Times of India. 15th August, 1, (2014).
- Choudhary S.R. Technical Working Group Meeting on Regional Action Plan and Targets for Prevention and Control of Non-communicable Diseases. Bangkok, Thailand, 7, (2013).
- Radhika G., Sathya R.M., Sudha V., Ganesan A. and Mohan V. J. Assoc. Phys. Ind., 55, 405-411, (2007).
- Jan R.A., Shah S., Saleem S.M., Waheed A., Mufti S., Lone M.A. and Ashraf M. J. Assoc. Phys. Ind., 54, 22-26, (2006).
- Ghosh A, Sarkar D, Mukherji B, Pal R. Ann. Trop. Med. Pub. Health., 6, 71-5, (2013). Available from: http://www.atmph.org/text.asp?2013/6/1/71/115209
- Mohan S. and Prabhakaran D. Technical training group meeting on regional action plan and targets for prevention and control of non communicable diseases Bangkok, Thailand. WHO, (2013).
- World Health Organization. Report of the Regional Meeting, New Delhi, India. 11–13 December 2012.
- He F.J., Pombo-Rodrigues S., and Macgregor G.A. BMJ Open, 4(4), e004549, (2014).
- Webster J., Dunford E., Kennington S., Neal B., and Chapman S. Pub. Health. Nutr., 17(1),212-8 (2014,).
- UNCTAD. Transnational corporations, agricultural production and development. World Investment Report, (2009).
- UNIDO. Agro-value chain analysis and development. The UNIDO Approach Working Paper, (2009).
- Srinivasan N. Workshop on Enhancing Exports’ Competitiveness Though Value Chain Finance. Supported by the Indian Trust Fund, Ministry of Finance, Government of India. Background Paper Series 1-7. Background Paper 3, (2012)
- CTAC. Reformulation of products to reduce sodium: Salt reduction guide for the food industry, (2009).
- He F.J., and MacGregor G.A. J Hum Hypertens, 23,363‐84, (2009).
CrossRef - Jayadevan G.R. Abhinav, 1, 8-15, (2012).
- Centers for Disease Control and Prevention. Improving the Food Environment through Nutrition Standards: A Guide for Government Procurement. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Division for Heart Disease and Stroke Prevention, (2011).
- Food Standard Agency. Available from: http://webarchive.nationalarchives.gov.uk/20131104005023/http://www.food.gov.uk/multimedia/pdfs/citforumfop.pdf
- Bureau of Nutritional sciences, Food Directorate, Health Products and Food Branch, Health Canada, (2012).

This work is licensed under a Creative Commons Attribution 4.0 International License.






