

Introduction
As the human population is becoming more and more sensitive to a wide array of diseases, including a huge rise in lifestyle disorders such as hypertension, diabetes, obesity, and cancer, the awareness regarding food as a means of disease prevention and treatment is increasing. Consequently, the use of food and dietary supplements as preventive and therapeutic agents is being actively studied all over the world. Most such studies to date have been focused on individual nutrients and their effects on the human body, but studying the interaction between nutrients in food and the human body is extremely important to ensure adequate nutrition to the body and the prevention of diseases. The nutrients mainly affect the human body either directly or through interaction with other nutrients. The interactions between nutrients can be synergistic, which brings about maximum benefit to the host, or antagonistic which is one nutrient negatively affects the absorption and bioavailability of other nutrients in the body.1,2 It is very important to gain insights into these interactions, particularly synergistic type, to harness their positive health benefits and to ensure that the body receives appropriate nutrition. According to Jacobs and his co-workers, the food synergy concept focuses on these synergistic interactions, among dietary patterns, food and food components that produce cumulative or more than cumulative effects on the health3. In many studies, it has been found that individual or isolated nutrients are not as effective as whole foods against diseases; such findings align with the concept of food synergy.3 Similarly, in comparison with individual foods, consuming a synergistic combination of foods provides greater health benefits.4 Additionally, understanding food synergy is also essential for nutrition science personnel so that maximum benefit from the micronutrients can be derived, and any side effects from unsafe nutrient combinations can be prevented.
Since most dietary advice focuses on individual nutrients, the nutrient–nutrient interactions are often ignored. However, the concept is very clear that the nutrients interact chemically and biologically. The Nutrition Society Spring Conference, 2018, one research highlighted the need to advance research to comprehend not only the outcomes of individual nutrients but also their interactions and significance for physiological function, and ultimately well-being.5 Micronutrient synergies are majorly categorized into three types: mineral-mineral synergy, mineral-Vitamin synergy, and Vitamin-Vitamin synergy.
Mineral-mineral synergy
This type of synergy mostly occurs at the metabolic level. The most common example of such synergy is the interaction between iron and copper: sufficient concentration of copper in the body is needed for proper iron utilization, and any deficiency of copper hampers iron metabolism in body.6 Some of the known synergistic mineral-mineral interactions include the interaction between potassium, magnesium, and calcium; the combination when consumed together, can help lower blood pressure and decrease the chances of getting a stroke.7 Also, the synergistic interaction between potassium and sodium lower/maintains the blood pressure8. Selenium and iodine work in synergy9 in the synthesis and metabolism of thyroid hormone, and for the normal functioning of the thyroid gland.10
Vitamin-Vitamin synergy
Vitamins are essential for multiple body functions and their maintenance. They function as coenzymes and are involved in the absorption and metabolism of different nutrients, mainly
proteins, carbohydrates, and fats. Vitamins are synergistically engaged with each other in many enzymatic reactions.1,11
Vitamin-mineral synergy
The synergy between Vitamins and minerals has been identified in a variety of metabolic functions. This interaction takes place in a variety of ways: action of the Vitamins on mineral metabolism, the action of minerals on Vitamin metabolism, and their combined role in the protection of the body.1,4
The synergistic effect of micronutrients can provide multiple benefits to the body. For instance, it increases the bioavailability of nutrients.4 Vitamin E and Vitamin C act synergistically to improve each other’s absorption.1 Similarly, Vitamin C increases iron absorption in the body.12,4 The idea of food synergy in the context of micronutrients is highly reliant on bioavailability. The knowledge of nutrient bioavailability can help and formulate dietary recommendations for synergistic foods that can easily be accepted by the general population.4 Moreover, the micronutrient synergy is proving to be helpful in the treatment and prevention of non-communicable chronic diseases, such as diabetes mellitus, cardiovascular diseases, obesity, and cancer; and, research is intensively being conducted to build the evidence-based foundation for such claims.4 Micronutrient synergy regulates low-density lipoprotein (LDL) levels,13, 14 improves blood circulation and reduces inflammation in the heart.15 Vitamin D and Vitamin K synergy improve blood glucose metabolism in diabetic patients by promoting insulin secretion from the pancreas and stimulating the insulin receptor genes.4 Certain micronutrient combinations also play a key role in cancer prevention, for example, Vitamin A and zinc decreases the risk of non-cardia stomach cancer.4 There has always been a link between immunity, infection and nutrition. A lot of diseases hamper nutrient absorption and thus make the body less immune against future infections. This way the body enters in the vicious cycle of infection and malnutrition. Some synergistic food combinations act as immune boosters and help maintain a healthy immune system.16, 17 Vitamins C and D, along with zinc, are the micronutrients which showed the synergistic support for immune system.17 Consumption of a nutrient in a concentrated or bolus form as a supplement may have unintended gastrointestinal effects. Food and micronutrient synergy by its buffering and competitive actions can control the entry and absorption of nutrients in the human body and thus can prevent such adverse effects.2 We have mentioned several examples of the micronutrient synergy (mineral-mineral, Vitamin-mineral, and Vitamin-Vitamin) showing their importance human health. The concept of food and nutrient synergy needs to be actively explored and researched, because this will inform and influence populations about key role played by healthier food choices and dietary patterns in preventing and treating lifestyle-related disorders. With this background, we systematically reviewed synergistic relationship in between Vitamins D and K on the cardiovascular health and the maintenance of bone health.
Vitamin D
It is a fat-soluble Vitamin and also a prohormone, which acts as a precursor for hormone having important function in calcium and phosphate metabolism.18 It is chemically known as calciferol and comprises of D2: ergocalciferol and D3 : cholecalciferol. The Figure 1 shows the various structures of Vitamin D.
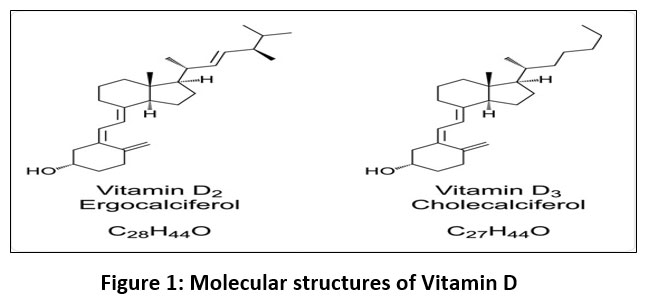 |
Figure 1: Molecular structures of Vitamin D |
There are very few natural sources of Vitamin D, therefore we have to fortify them with to counter the global issue of Vitamin D deficiency.19 The synthesis of Vitamin D occurs with the exposure of body to sunlight. Basically, it is synthesized in skin, liver, and kidney and can be understood by the Figure 2.20
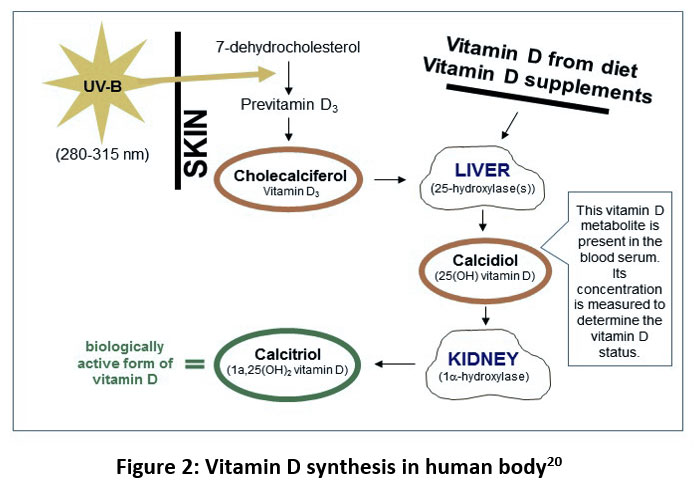 |
Figure 2: Vitamin D synthesis in human body20 |
In human body, the Vitamin D synthesis starts from the skin with exposure to ultraviolet-B (UV-B) solar radiation (280-315 nm), which converts 7-dehydrocholesterol to preVitamin D3, which then isomerizes into Vitamin D3 or cholecalciferol. Vitamin D3 synthesized through skin or taken through supplements and foods are further metabolized into calcidiol or 25-hydroxyVitamin D (25(OH)D) in liver by 25-hydroxylase enzyme. 25(OH)D is further converted in the kidneys to 1,25-dihydroxy Vitamin D or calcitriol, which is the main hormonal form of Vitamin D and is responsible for most of its biological functions. Vitamin D level in the body is generally determined by measuring the serum level of calcidiol.
Vitamin D has several significant functions in the body. For instance, it performs crucial role in blood calcium regulation. Calcitriol, the active metabolite of Vitamin D, increases calcium and phosphorus absorption by intestine and simultaneously reduces calcium excretion from kidneys. It contributes to calcium deposition in the bones in indirect way.21 It plays pivotal role in proper functioning of immunomodulatory properties of the body.22 Calcitriol inhibits PTH (parathyroid hormone) secretion from the parathyroid glands.22 It also controls growth of parathyroid gland.23 It might be vital for the prevention and treatment of extra-skeletal diseases including cancer24 There have been a lot many researches that are focused on the concept that Vitamin D can reduce diabetes risk by influencing various pathways involved in the patho-physiology of type 2 diabetes mellitus, including dysfunction of pancreatic β-cells, decreased insulin action, and systemic inflammation.25 The fact that the receptors of Vitamin D have been identified in almost all immune cells and calcitriol (Vitamin D’s biologically active form) can modulate immune responses, further led scientist to link the deficiency of Vitamin D with the increasing prevalence of autoimmune diseases.26
Vitamin K
It is a fat-soluble Vitamin and was initially known as “koagulation” (coagulation) Vitamin, because upon discovery, it was found that the vitamin was essential for preventing fatal haemorrhage by promoting normal blood clotting.21 It exist is in two naturally occurring forms: Phylloquinone (K1) and Menaquinone (K2) (Figure 3). Menadione, which is known as Vitamin K3, is a precursor for Vitamin K2 / menaquinone.
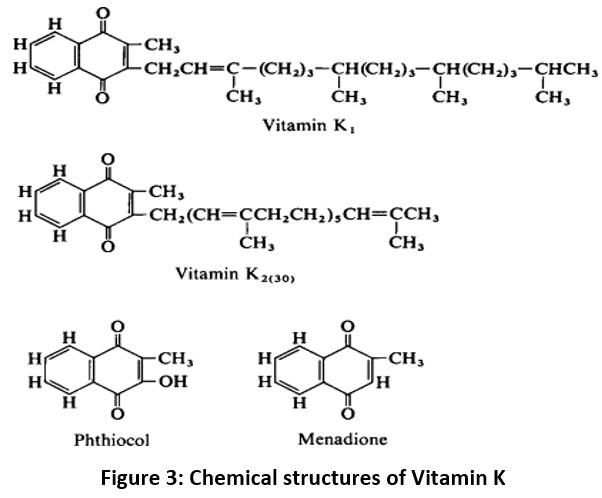 |
Figure 3: Chemical structures of Vitamin K |
Nutritional source of Vitamin K, particularly phylloquinone, is green leafy vegetables. On the other hand, menaquinones can be found in trace quantities in a number of fermented and animal-based foods. Bacteria in the human gut produce almost all menaquinones, particularly the long-chain menaquinones.27 Vitamin K provides several functions to the human body. For instance, it facilitates the synthesis of blood clotting factors in liver by acting as a cofactor for enzymes that convert prothrombin into thrombin21. Vitamin K is essential for the metabolism of bone.28 Osteocalcin, a calcium-binding protein in bone, is synthesized with the help of Vitamin K.29 Low intake of Vitamin D or low levels of circulating Vitamin K have been linked with low BMD and can increase the chances of hip fractures in women.21 It also reduces osteo-clastogenesis (the formation of bone resorbing cells).30
Very few systematic studies have been conducted on the Vitamin-Vitamin synergism. The present endeavour has been planned to assess the synergistic effect of two most important vitamins as D and K supplementation on the bone and cardiovascular health.
Methodology
The present systematic review complied with the recommendations specified in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). We used online research database platforms PubMed and Google Scholar for extracting studies. The search was restricted to the studies published from 2006 to 2021 (i.e., the past 15 years) in English language. Table 1 showed the PICOS (inclusion and exclusion) criteria used during the systematic review.
Table 1: Study Selection Criteria.
| PICOS | Inclusion Criteria | Exclusion Criteria |
| Participants | Human subjects | Animal subjects or animal model-based studies |
| Intervention | Vitamin D & Vitamin K supplementation | Any other supplementation |
| Outcome | Improved Bone Health and Cardiovascular Health | Any other outcome |
| Study setting | Experimental studies: Randomized controlled trials and clinical trials; cohort studies | Reviews |
The search strategy devised as per the PRISMA guidelines involved thorough review of the titles and abstracts, then review of the entire document articles. The screening of studies was grounded on the PICOS inclusion and exclusion criteria decided at the start of the study. For this systematic review, the relevant studies were extracted from the online research database platforms by using the main key words – “Vitamin D and Vitamin K” related with their “synergy”, “interaction”, “supplementation”, “supplementation improved bone health”, “supplementation reduced fractures”, “supplementation improved osteoporosis”, “supplementation for heart health”, and “cholecalciferol and phylloquinone”. The initial database search returned 497 articles (Figure 4), including 436 articles from PubMed and 61 articles from Google Scholar. Out of the total 497 articles, we removed 35 articles that were found to be duplicate. The remaining 462 studies were further screened by reading titles and abstracts, and it yielded 16 articles for full-text review. Out of these 16, we further excluded 4 studies due to various reasons: insufficient data, editorial, and intervention not matching the inclusion criteria. Therefore, finally, 12 studies were selected for the qualitative analysis. From the included studies, following information was collected: study design, number of participants, age range of the participants, duration of the study, general health of the participants, intervention given or parameters observed, and outcome of the study.
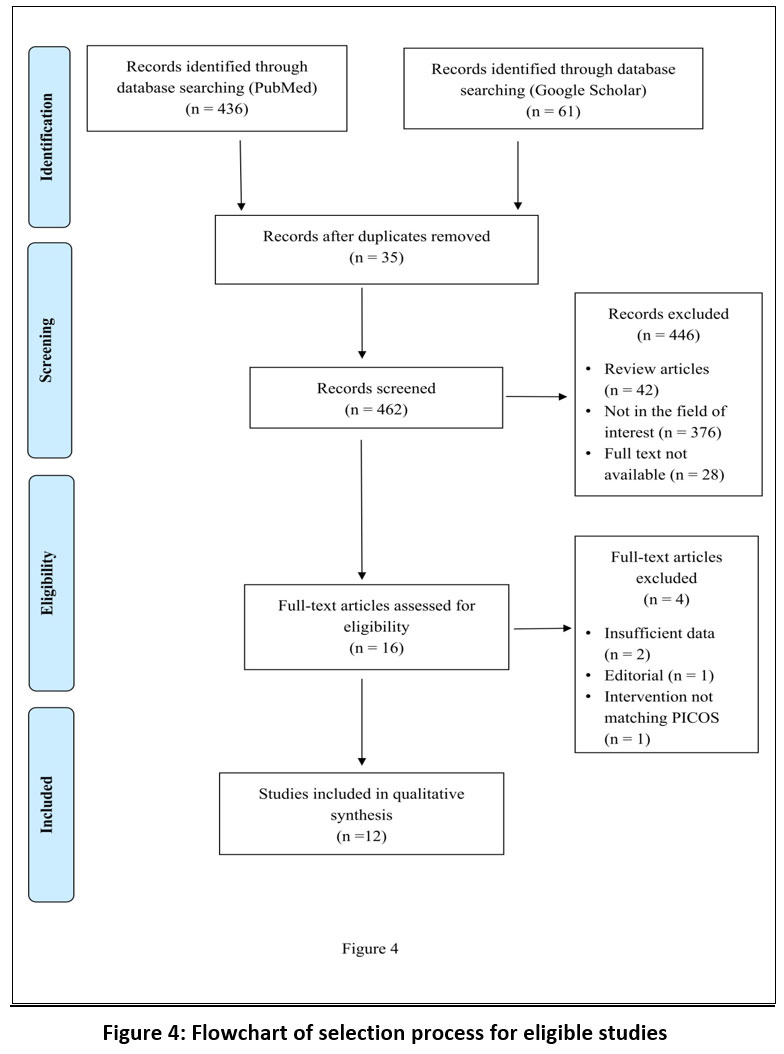 |
Figure 4: Flowchart of selection process for eligible studies |
Results
As per the exclusion and inclusion criteria, 16 studies were retrieved for full text screening. Out of these 16 studies, 12 met the inclusion criteria. Out of the 12 included studies, 5 of them were randomized controlled trial, 6 were observational studies, and 1 was interventional studies. Most (four) of the studies were conducted in the Netherlands, two in Denmark, and one each in Canada, Czech Republic, Iran, Turkey, the United States, and the United Kingdom. Table 1 summarizes a component of the systematic review. The study reported to have 20 to 5544 participants. The 12 studies reported data from a total of 8216 participants whose age range varies from 3 years to 85 years and included both males and females. Out of the 12 studies, 5 included healthy participants31-35, one study included post-menopausal women36, one study did not mention the health status of the participants37, whereas 5 included data from patients with different medical conditions: classical galactosemia38, thalassemia major patients suffering from Thalassemia Osteopathy (TSOP)39; patients suffering from diabetes along with Coronary Heart Disease (CHD)40 ; patients exhibiting clinically significant depression symptoms and one or more functional limitation 41 ; and patients with Celiac Disease (CD).42 Out of the 12 studies, 8 studies31, 32, 35, 36, 38, 39, 42 examined the synergistic relationship of Vitamin D and K upon the bone development, whereas 4 studies33, 34, 37, 40 assessed their synergistic effect on cardiovascular health.
Results were interpreted based on improved bone health by assessing the progress in BMC, lower extremity function, BMD, and bone turnover, on the other hand improvement in cardiovascular health was evaluated based on CIMT, arterial stiffness, hypertension, and cardiac structure. After summarizing the randomized controlled trials and clinical trials, the Table 2.
Also focuses on the cohort studies and observational prospective studies based upon their synergistic relationship. The summary of the individual studies has been discussed below”
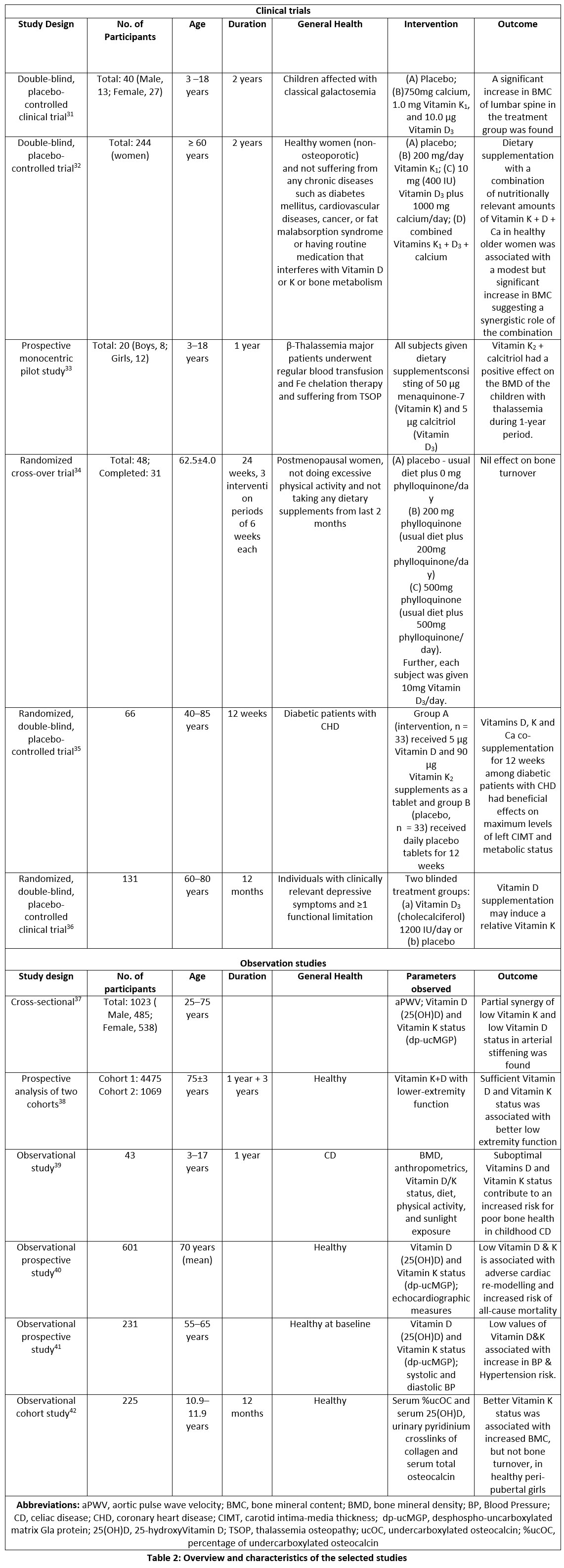 |
Table 2: Overview and characteristics of the selected studies. |
Improvement in bone health
Eight out of the 12 studies were focused on finding the possibility of increasing BMD or bone turnover by combining Vitamin D and Vitamin K. These studies included participants of different age groups and took into consideration other medical conditions or co-morbidities as well. Seven out of the 8 studies showed improvement in bone health by way of increase in BMD. According to Bügel and his co-workers, no significant improvement in bone restoration was observed in post-menopausal women.36 One more research work showed that both supplementations helped elderly persons with their lower extremity function32. After analyzing the results of the 8 studies, it can clearly be concluded that their combination showed synergistic effect on bone health in all age groups with various medical conditions such as CD, galactosemia, symptoms of depression and functional impairment, and, on the bone health in post-menopausal women.
The research conducted by Panis and his colleagues 38 worked upon the impact Vitamin D, K and Ca on the bones of classic galactosaemic children. One of the complications of galactosemia in children is the decreased BMD and an inadequate deposition of bone mass, which can promote osteoporosis and fractures later in life. Vitamin D3 is essential for bone development and functions in a variety of ways to aid calcium absorption. Similarly, as discussed before, Vitamin K1 is equally essential in bone metabolism, a placebo-controlled, double-blind study having 2-year clinical trials with two groups. One group received placebo and the second received daily two tablets containing 5 µg Vitamin D3, 0.5 mg of Vitamin K1, and 375 mg calcium. The following factors were analyzed at baseline and after in the beginning of the study and then after a year of treatment: BMC and body composition data; 1,25-dihydroxy Vitamin D (1,25OHD); markers of bone development under-carboxylated and carboxylated osteocalcin (ucOC and cOC respectively); bone resorption markers, such as amino terminal telopeptide and carboxy terminal telopeptide; and the bone re-modelling marker insulin-like growth factor-I, total zinc, magnesium, phosphorus and calcium. When compared with the controls, children who received calcium along with Vitamins K1 and D3 supplements had shown significant improvement in BMC of the lumbar spine. This results the synergistic outcome highlights the impact of Vitamin D and K on BMD.
Bolton-Smith’s study31, which was a random controlled study conducted for 2 years, focused over the role of both the Vitamins on the BMC of healthy women older than 60 years. The study consisted of 4 groups in which 244 participants were randomly assigned. A placebo was administered to one group, the second group received only Vitamin K1 (200 mg per day), group 3 received Vitamin D3 (400 IU per day) and calcium (1000mg), whereas the last group (i.e., group 4) received a combination of calcium, Vitamin D3 and Vitamin K1 at the same levels as in group 2 and 3. The key finding of the study showed the dietary supplementation with a proper combination of nutritionally required levels of Vitamin K, D, and Ca was linked to significantly small increase in the BMC at trabecular bone among healthy old aged women. The similar changes were not noticed among either the Vitamin K or calcium plus Vitamin D group implying that the combination of Vitamins has a synergistic effect.
In a prospective mono-centric pilot study by Ozdemir and co-workers39, they investigated the impact of Vitamin K2 and D supplements upon patients having Thalassaemic Osteopathy (TOSP), (including both osteopenia and osteoporosis). The 20 subjects included in the study were children aged between 3 and 18 years and were affected with β-thalassemia. All subjects were given a dietary supplement consisting 50 mg menaquinone-7 and 5 mg Vitamin D3 for 1 year. The combination of Vitamin K2 and Calcitriol showed strong positive impact upon BMD of lumbar spine of thalassaemic children over a one-year period.
Bügel and co-workers 36 conducted a 2-year study on 31 post-menopausal women based on the exclusion and inclusion criteria. It was a three-stage, randomised cross-over intervention research. The groups were as follows: (A) Placebo (common diet without any known the rapeuti value) (B) supplementation of 200 mg phylloquinone (common diet with supplementation of 200 mg phylloquinone/day); (C) supplementation of 500 mg phylloquinone (common diet with supplementation of 500 mg phylloquinone/day).
Further, each subject was given 10 µg (400 IU) Vitamin D3/day. Different blood, urine, and bone factors were assessed during the course of investigation. Analysis of the parameters proclaim an increase in Vitamin K status after the intervention. Although, the supplementation of phylloquinone in postmenopausal women significantly decreased the ucOC, although, No significant difference had been observed on bone turnover of the post-menopausal women during and after the course of study.
Van Ballegooijen and co-workers 41 carried a randomised, double-blind, placebo-controlled clinical trial to determine the impact of Vitamin D supplementation on Vitamin K status by assessing the plasma matrix GLA protein, which is a biomarker of functional Vitamin K status.43 The participants in the study of 60 to 80 years of age and were suffering from major clinical depressive indications and functional limitations. The primary result showed no significant increase or improvement in Vitamin K status after 6 months. However, when the results were sensitively analyzed by excluding multiVitamin users and Vitamin K antagonists, the difference between the two intervention groups was significant, i.e., there was an increase in the concentration of des-phospho-uncarboxylated matrix Gla protein (dp-ucMGP) and ultimately deficit in Vitamin K and consuming the supplements of Vitamin D. This implies that a synergy exists between Vitamin K and Vitamin D.
Shea and co-workers 32 analyzed two independent cohorts vitamin D & K for better function of the lower part of the body. In one of the cohort, nutrient status was assessed by measuring Vitamin levels in the blood and Vitamin K, whereas in other cohort, the assessment of nutrient status was done with the help of Food Frequency Questionnaires (FFQ). In the study 1, the lower-extremity function was evaluated using 20-metre gait speed and a SPPB (Short Physical Performance Battery), in contrast in study 2, the functionality of the lower extremities was evaluated using the standard method. In the analysis it was found that participants with sufficient amount of both the vitamins had better test scores for the lower-extremities function. This study proved the synergistic benefit of both the Vitamins on bone and joint functioning, which suggests that the co-supplementation can help in the treatment and prevention of knee osteoarthritis.
In an observational trial, Mager and colleagues42 investigated the relationships between BMD and Vitamin D and Vitamin K status in kids and adolescents. Kids with CD were having increased risk of low BMD caused due to several factors such as – inadequate nutritional intake due to having gastrointestinal problems (pain, diarrhoea, and nausea), a low ability to absorb fat-soluble Vitamins and the occurrence of chronic inflammation, which impairs bone metabolism.39 Different blood parameters, such as markers of Vitamin D and K sufficiency as well as BMC and BMD were assessed at baseline (i.e., as soon as CD was diagnosed) and after 1 year of following GFD. Analysis revealed that children with CD are more likely to have poor bone health when they are deficient in Vitamin D as well as Vitamin K+), demonstrating a synergistic effect between the two nutrients.
In an association study conducted by O’Connor and co-workers35 among 223 Danish girls (11 – 12 years), investigated associations between the status of K indicator serum %ucOC (undercarboxylated osteocalcin) and BMC and biochemical markers of bone turnover.
The authors selected this age group because the peri-pubertal stage is considered as a complicated stage of bone formation, so it gives a crucial window of opportunity for the status of Vitamin K to alter the health of developing bones in children.
In this study, the estimation of the status of Vitamin K was done by the means of serum %ucOC, while the intakes of Vitamin D and calcium were calculated through dietary assessments using food frequency questionnaires. The BMC of the entire body and the lumbar spine were found to be positively correlated in this study which was conducted among 11–12-year-old girls with improved Vitamin K status, which was indicated by a lower percent ucOC.
Improvement in cardiovascular health
Four out of the 12 studies investigated the influence of consuming Vitamin D and K supplements together upon the cardiovascular health. The studies assessed different cardiovascular parameters such as arterial stiffness, systolic pressure and diastolic pressure, hypertension, and cardiac remodelling. All the studies proved that combination of Vitamin D with Vitamin K indeed exert a positive effect on cardiovascular health by improving either the arterial stiffness or the systolic pressure and diastolic pressure values.
In the cross-sectional research of Mayer and co-workers37 also explored consortium low Vitamin K and D status in facilitating arterial stiffness. The study was built upon the existing studies that have shown correlation among Vitamin D (or Vitamin K) alone and (with) arterial stiffness. In contrast this study aimed to explore associative effects of Vitamin D and K on arterial stiffness. The status of Vitamin K was assessed by estimating dp-ucMGP level, a sensitive marker that is only formed when the body is deficient in Vitamin K. It has also been found that there is a positive corelation between dp-ucMGP and degree of coronary calcification, which depicting the role of Vitamin K in heart health.44 On the other hand, Vitamin D levels were assessed by measuring 25-hydroxyVitamin D3 concentration in the blood. A measure of arterial stiffness called Aortic Pulse Wave Velocity (aPWV) was employed as a predictor of morbidity and mortality from cardiovascular complications.45 It was found in the study that subjects with low levels of Vitamin D and Vitamin K had an aPWV that was around seven times higher than that of subjects with levels in the highest quartile for both the Vitamins.
One of the studies conducted by Asemi and co-workers 40 to determine the impact of co-supplementing Vitamin D, K, and calcium on CIMT, glycemic control, lipid concentrations, and biomarkers of inflammation and oxidative stress in type 2 diabetic and overweight CHD patients.
It was based on previous studies that had shown the positive impact of both the Vitamins D and K on CIMT, inflammation, atherosclerosis, as well as insulin resistance independently. Study planed was a randomised, double-blind, placebo-controlled trial which was conducted with two treatment clusters for a period of 12 weeks. Cluster A (the intervention cluster) received a tablet containing Vitamin D (5 μg) and Vitamin K2 (90 μg), while Group B received placebo tablets.
In the study, the primary outcome was CIMT, on the other hand glucose homeostasis, biomarkers of oxidative stress and inflammation, and lipid profile were kept as secondary outcomes.
The consecutive co-supplementation of Vitamin D, K and calcium for 12 weeks helped in improving extremely high left CIMT levels, glycemic parameter, and HighDensity Lipoprotein (HDL) cholesterol levels in the patients of diabetes mellitus with stable CHD, however, it had no impact on the highest levels of CIMT (right), left and right CIMT (mean levels), other lipid profiles and oxidative stress indicators.
The relationship between Vitamin D and K levels and subclinical indicators of cardiovascular health was examined in one of the studies conducted by Dal Canto et al.33. There were 601 Hoorn study participants in this observational prospective study. Statistical analysis of the study revealed that the subjects with low levels of both the Vitamins (D and K) observed a defect in cardiac structure which was a major threat of all-cause deaths as compared to the subjects had normal status of Vitamin D and Vitamin K.
The main conclusion of the research study showed that Vitamin D was synergistically associated with Vitamin k in terms of cardiac function and all-cause mortality. But in order to corroborate the study’s findings, the authors recommended conducting additional extensive clinical investigation.
Van Ballegooijen and co-workers 34 conducted an observational prospective study to examine the joint relationship between poor Vitamin status (D and K), BP and Hypertension, which are risk factors for cardiovascular disease. For conducting the study, the data were extracted from a sample of 231 participants from second LASA cohort (Longitudinal Aging Study Amsterdam), which was conducted in 2002-2003 among 55- to 65-year-old adults, and the last follow up was done in 2011-2012. The following parameters were assessed to understand the association: plasma dp-ucMGP concentrations level of Vitamin K, serum 25(OH)D concentrations, level of Vitamin D, hypertension, total cholesterol, serum creatinine, and parathyroid hormone level. It was found out that participants with low levels of Vitamin D and K had significant increase in their systolic and diastolic blood pressure as compared with the reference that is the group with adequate levels of Vitamin D and Vitamin K status. Similar pattern was also found between low Vitamin D and low Vitamin K combination and incident hypertension; however, the association was not statistically significant.
In conclusion, all studies (apart from one) demonstrate that Vitamin D and Vitamin K work synergistically and have a critical role in the prevention of bone fractures, poor BMD, and cardiovascular diseases.
Discussion
The present systematic review has broadly identified evidences for the synergistic relationship between the status of Vitamin D and K status on bone and cardiovascular health. The studies included in the systematic review differed considerably in study designs (randomized controlled trials, observational studies, and interventional studies), number of participants, baseline characteristics of the participants, and geographical settings. All the studies (excluding one) show that Vitamin D and Vitamin K work in synergy and have a significant role in preventing bone fractures, low BMD, and cardiovascular disorders. The studies also vary substantially in the Vitamin D and K dosage regimen given as supplementation. The doses of Vitamin K1 supplements in the studies varied from 200 µg to 1000 µg per day; in contrast the dose for Vitamin K2 supplements ranged from 50 µg to 90 µg. Similarly, among the studies, the quantities of Vitamin D supplements were ranged between 5 and 30 µg per day. Both isoforms (or vitamers) of Vitamin K (Vitamin K1 and Vitamin K2) have been used by the studies for supplements: 3 studies gave Vitamin K131, 36, 38 whereas 2 studies used Vitamin K2, i.e., menaquinone-7 or MK-7.39, 40 Vitamins K1 and K2 differ in their dietary source, cellular absorption rates, tissue distribution, bioavailability, functions, and target activity.46, 47 Therefore, a proper care must be taken in selecting one over other as a supplement with Vitamin D for bone and cardiovascular benefits. Osteoporosis is indeed a huge communal health concern all over the world. Its prevalence has been steadily increasing, with new figures indicating that it affects more than 200 million people worldwide.48 Vitamin D deficiency and calcium deficiency are also important risk factors for osteoporosis. Sufficient Ca and Vitamin D intake has been essential during the prevention and treatment of osteoporosis and associated damages. A lack of Ca / Vitamin D results in decreasing the calcium absorption and increasing the bone re-modelling and, which leads to significant bone loss. Neuromuscular dysfunctions such as muscle fatigue and a higher risk of falling have also been connected to low Vitamin D levels in the blood. Furthermore, it has been demonstrated that combining Vitamin D with other nutrients, such as Vitamin K, can reduce the likelihood of fractures by increasing BMD and improving bone structure.
As per the growing evidence, Vitamin K, both independently and synergistically with Vitamin D have favourable impacts on calcium metabolism. The findings of epidemiological and clinical studies point to a new dietary model for calcium distribution that involves co-supplementation of both the fat-soluble vitamins. Most studies included during the present qualitative analysis showed the combination of Vitamin D and K intervention (sometimes with calcium as well) has an important and favourable outcome related to bone health as well as cardiovascular health when compared with single nutrient supplementation, i.e., either Vitamin D or Vitamin K independently or placebo groups. This research backs up the theory that Vitamin K and Vitamin D (both the Vitamins) work synergistically to prevent bone loss. Vitamin K2 has been shown in clinical trials to be effective as a means of managing osteoporosis and the avoidance of fractures independently.49 Considering the few research that have been included in the present systematic review, joint supplementation can also improve cardiovascular health. It is worth noting that there have been limited clinical trials on the synergistic effects of both the Vitamins on human health. Moreover, in most of the studies included here, Vitamin D and K supplements were often mixed with other micronutrients such as calcium, making it complex to isolate the influence of Vitamin D and K. Similarly, the exact physiological processes underlying the relationship between Vitamin K and Vitamin D-related homeostasis are still unexplained and most of the studies included in this review did not venture into identifying the processes following the synergistic relationship of both the Vitamins D and K. However, some studies have speculated the possible mechanism of this synergy: (1) Matrix Gla protein (MGP) is a Vitamin K-dependent protein with implication in cardiovascular system maintenance. The gene that encodes MGP contains Vitamin D responsive element in its promoter region, and Vitamin D has been shown to increase MGP mRNA expression in humans50; (2) The co-administration of both the Vitamins in animal studies has been found out to increase the bone formation marker levels like osteocalcin in a time-dependent fashion.51
Conclusion
This systematic review showed that combination of Vitamins D and K can improve various parameters of bone health and cardiovascular health in different population, thus emphasizing the importance of Vitamin-Vitamin synergy. Because optimum levels of both the Vitamins are necessary for maintaining proper body functions, the present findings recommend further research on combining Vitamins D and K as a potential therapeutic strategy for improving bone and cardiovascular health. Unfortunately, most trials have studied Vitamin D either alone or in low-dose (400–800 IU daily), which had been found by some studies to have little to no effect on BMD, bone turnover, and fracture prevention in some population such as postmenopausal women.36, 52 Recently, a randomized, double-blind, placebo-controlled clinical trial, known as Vitamin D and OmegA-3 TriaL (VITAL), with 25871 participants used cholecalciferol supplementation at a higher dose of 2000 IU/d, with mega-3 fatty acids eicosapentaenoic acid and docosahexaenoic acid, 1 g/d53. However, the supplementation did not find any significant effect on cardiovascular outcomes of the participants. The VITAL trial was targeted on the Vitamin D supplementation due to which the study did not use other Vitamins in combination with Vitamin D. The future clinical trials involving co-supplementation of more than one Vitamin with various dosage regimen can be an attractive research area for scientists. Therefore, research on food synergies are the emerging technologies in food science and nutrition and this unexplored side has to be fully explored for the beneficial of human kind54.
An additional concern is that neither a cut-off value for Vitamin K status nor for Vitamin K supplementation is currently known. When research was planned and conducted to confirm the synergistic effects of Vitamins D and K is more conclusive, and it has provided yet another reason to consume a diet rich in fermented dairy products and fresh vegetables for development and strength of bone and heart health. Both Vitamins D and K are, in principle, ideal for the population-based primary prevention of chronic diseases due to their safety, relatively in-expensive price, and easy availability. Before larger therapeutic decisions can be made, more scientific evidences on the possible interplay between Vitamin D and Vitamin K metabolism are extremely required. Further research will also be helpful to assess the long-term effects of high-dose Vitamin D supplementation and the role of Vitamin K and Vitamin D combination on bone and cardiovascular functions.
Acknowledgment
The authors are grateful to Dr. V.K. Modi, Director, Amity Institute of Food Technology, Amity University, Uttar Pradesh, for his expertise and guidance throughout all the aspects of the study.
Conflict of Interest
The authors have no conflicts of interest to declare.
Funding of Sources
The study was not supported by any research funding.
Authors’ contributions:
Vinita Singh – Conception and design of the study, Data curation, Investigation, Methodology, Writing – original draft, Visualization
Shravali Jain – Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Visualization.
Satya Praksah – Data curation, Investigation, Methodology
Monika Thakur – Conceptualization, analysis and interpretation of data, Methodology, Validation, Writing – review & editing, Supervision.
References
- Tripathy S. Interrelationship of micronutrients: Antagonism and synergism. Int J Pure Appl Biosci. 2017;5(6):208-214. doi:10.18782/2320-7051.5835.
- Jacobs D. R., Gross M. D., Tapsell L. C. Food synergy: An operational concept for understanding nutrition. Am J Clin Nutr. 2009;89(5):1543S-1548S. doi:org/10.3945/ajcn.2009.26736B.
- Jacobs D. R., Tapsell L. C., Temple N. J. Food Synergy: The key to balancing the nutrition research effort. Public Health Rev. 2011;33:(2)507-529. doi:org/10.1007/bf03391648.
- Natarajan T. D., Ramasamy J. R., Palanisamy K. Nutraceutical potentials of synergic foods: A systematic review. J Ethn Foods. 2019;6:27. doi:org/10.1186/s42779-019-0033-3.
- Combet E., Gray S. R. Nutrient-nutrient interactions: Competition, bioavailability, mechanism and function in health and diseases. Proc Nutr Soc. 2019;78(1):1-3. doi:org/10.1017/S0029665118002732.
- O’Dell B. L. Mineral interactions relevant to nutrient requirements. J Nutr. 1989;119(12suppl):1832-1838. doi:org/10.1093/jn/119.12_suppl.1832.
- Iqbal S., Klammer N., Ekmekcioglu C. The effect of electrolytes on blood pressure: A brief summary of meta-analyses. Nutrients. 2019;11(6):1362. doi:org/10.3390/nu11061362.
- Morgan T., Myers J., Teow B. H. The role of sodium and potassium in the control of blood pressure. Aust N Z J Med. 1984;14(4):458-462. doi:org/10.1111/j.1445-5994.1984.tb03615.x.
- Cann S. A., Van Netten J. P., Van Netten C. Hypothesis: Iodine, selenium and the development of breast cancer. Cancer Causes Control. 2000;11(2):121-127. doi:org/10.1023/A:1008925301459.
- Schomburg L., Köhrle J. On the importance of selenium and iodine metabolism for thyroid hormone biosynthesis and human health. Mol Nutr Food Res. 2008;52(11):1235-1246. doi:org/10.1002/mnfr.200700465.
- Singh, V., Prakash, S., Thakur, M. Assessment of Food Synergies as a boon to Combat Iron Deficiency Anemia in Adolescent Girls. J Optoelec Laser. 2022; 41(7), 35–43.
- Vannucchi H. Interaction of Vitamins and minerals. Arch Latinoam Nutr. 1991;41(1):9-18.
- Chen C. Y., Milbury P. E., Lapsley K., Blumberg J. B. Flavonoids from almond skins are bioavailable and act synergistically with Vitamins C and E to enhance hamster and human LDL resistance to oxidation. J Nutr. 2005;135(6):1366-1373. doi:org/10.1093/jn/135.6.1366.
- Ros E. Health benefits of nut consumption. Nutrients. 2010;2(7):652-682. doi:org/10.3390/nu2070652
- Oude Griep L. M., Wang H., Chan Q. Empirically derived dietary patterns, diet quality scores, and markers of inflammation and endothelial dysfunction. Curr Nutr Rep. 2013;2:97-104. doi:org/10.1007/s13668-013-0045-3.
- Maggini S., Maldonado P., Cardim P., Newball C. F., Sota Latino E. R. Vitamins C, D and Zinc: Synergistic roles in immune function and infections. Vitam Miner. 2017;6(2):167 doi:org/10.4172/2376-1318.1000167.
- Gombart A. F., Pierre A., Maggini S. A review of micronutrients and the immune system–working in harmony to reduce the risk of infection. Nutrients. 2020;12(1):236. doi:org/10.3390/nu12010236.
- Kulda V. Vitamin D metabolism. Vnitr Lek. 2012;58(5):400-404.
- Wilson L. R., Tripkovic L., Hart K. H., Lanham-New S. A. Vitamin D deficiency as a public health issue: Using Vitamin D2 or Vitamin D3 in future fortification strategies. Proc Nutr Soc. 2017;76(3):392-399. doi:org/10.1017/S0029665117000349.
- Bundesamt für Strahlenschutz, BfS. The Vitamin D metabolism, https://www.bfs.de/EN/topics/opt/uv/effect/acute/Vitamin-d.html; [accessed 20 January 2022]
- Chadha R., Mathur P. Nutrition: A Lifecycle approach. Orient BlackSwan, 2015.
- Urena-Torres P, Souberbielle J. Pharmacologic role of Vitamin D natural products. Curr Vasc Pharmacol. 2014;12(2):278-285. doi:org/10.2174/15701611113119990020.
- Khundmiri S. J., Murray R. D., Lederer E. PTH and Vitamin D. Compr Physiol. 2016;6(2):561-601. doi:org/10.1002/cphy.c140071.
- Jeon S. M., Shin E. A. Exploring Vitamin D metabolism and function in cancer. Exp Mol Med. 2018;50(4):1-14. doi:org/10.1038/s12276-018-0038-9.
- Mitri J., Pittas A. G. Vitamin D and diabetes. Endocrinol Metab Clin North Am. 2014;43(1):205-232. doi:org/10.1016/j.ecl.2013.09.010.
- Bizzaro G., Antico A., Fortunato A., Bizzaro N. Vitamin D and autoimmune diseases: Is Vitamin D receptor (VDR) polymorphism the culprit? Isr Med Assoc Jour. 2017;19(7):438-443.
- Office of Dietary Supplements – Vitamin K. (2021, March 29). National Institute of Health, https://ods.od.nih.gov/factsheets/VitaminK-HealthProfessional/; [accessed 20 January 2022].
- Akbari S, Rasouli-Ghahroudi AA. Vitamin K and bone metabolism: A review of the latest evidence in preclinical studies. Biomed Res Int. 2018; 2018:4629383. doi:org/10.1155/2018/4629383.
- Hauschka P. V., Lian J. B., Cole D. E., Gundberg C. M. Osteocalcin and matrix Gla protein: Vitamin K-dependent proteins in bone. Physiol Rev. 1989;69(3):990-1047. doi:org/10.1152/physrev.1989.69.3.990.
- Palermo A., Tuccinardi D., D’Onofrio L., Watanabe M., Maggi D., Maurizi A. R., Greto V., Buzzetti R., Napoli N., Pozzilli P., Mnfrini S. Vitamin K and osteoporosis: Myth or reality? Metabolism. 2017;70:57-71. doi:org/1.0.1016/j.metabol.2017.01.032.
- Bolton-Smith C., McMurdo M. E. T., Paterson C. R., Mole P. A., Harvey J. M., Fenton S. T., Prynne C. J., Mishra G. D., Sheareer M. J. Two-year randomized controlled trial of Vitamin K1 (phylloquinone) and Vitamin D3 plus calcium on the bone health of older women. J Bone Miner Res. 2007;22(4):509-519. doi:org/10.1359/jbmr.070116.
- Shea M. K., Loeser R. F., McAlindon T. E., Houston D. K., Kritchevsky S. B., Booth S. L. Association of Vitamin K status combined with Vitamin D status and lower-extremity function: A prospective analysis of two knee osteoarthritis cohorts. Arthritis Care Res. 2018;70(8):1150-1159. doi:org/10.1002/acr.23451.
- Dal Canto E., Beulens J. W. J., Elders P., Rutters F., Stehouwer C. D. A., Van Der Heijden A. A., van Ballegooijen A. J. The association of Vitamin D and Vitamin K status with subclinical measures of cardiovascular health and all-cause mortality in older adults: The Hoorn Study. J Nutr. 2020;150(12):3171-3179. doi:org/10.1093/jn/nxaa293.
- Van Ballegooijen A. J., Cepelis A., Visser M., Brouwer I. A., Van Schoor N. M., Beulens J. W. Joint association of low Vitamin D and Vitamin K status with blood pressure and hypertension. Hypertension. 2017;69(6):1165-1172. doi:org/10.1161/HYPERTENSIONAHA.116.08869.
- O’Connor E, Mølgaard C., Michaelsen K. F., Jakobsen J., Lamberg-Allardt C. J. E., Cashman K. D. Serum percentage undercarboxylated osteocalcin, a sensitive measure of Vitamin K status, and its relationship to bone health indices in Danish girls. Br J Nutr. 2007;97(4):661-666. doi:org/10.1017/S0007114507433050.
- Bügel S., Sørensen A. D., Hels O., Kristensen M., Vermeer C., Jakobsen J., Flynn A., Mølgaard C., Cashmn K. D. Effect of phylloquinone supplementation on biochemical markers of Vitamin K status and bone turnover in postmenopausal women. Br J Nutr. 2007;97(2):373-380. doi:org/10.1017/S000711450715460X.
- Mayer O., Seidlerová J., Wohlfahrt P., Filipovský J., Cífková R., Černá V., Kučerová A., Pešta M., Fuchsová R., Topolčan O., Jardon K. M. C., Drummen N. E. A., Vermeer C. Synergistic effect of low K and D Vitamin status on arterial stiffness in a general population. J Nutr Biochem. 2017;46:83-89. doi:org/10.1016/j.jnutbio.2017.04.010.
- Panis B., Vermeer C., van Kroonenburgh M. J. P. G. , Nieman F. H. M., Menheere P. P. C. A., Spaapen L. J., et al. Effect of calcium, Vitamins K1 and D3 on bone in galactosemia. Bone. 2006;39(5):1123-1129. doi:org/10.1016/j.bone.2006.05.002.
- Ozdemir M. A., Yilmaz K., Abdulrezzak U., Muhtaroglu S., Patiroglu T., Karakukcu M., unal E. The efficacy of Vitamin K2 and calcitriol combination on thalassemic osteopathy. J Pediatr Hematol Oncol. 2013;35(8):623-627. doi:org/10.1097/MPH.0000000000000040.
- Asemi Z., Raygan F., Bahmani F., Rezavandi Z., Talari H. R., Rafiee M., et al. The effects of Vitamin D, K and calcium co-supplementation on carotid intima-media thickness and metabolic status in overweight type 2 diabetic patients with CHD. Br J Nutr. 2016;116(2):286-293. doi:org/10.1017/S0007114516001847.
- Van Ballegooijen A. J., Beulens J. W. J, Schurgers L. J., de Koning E. J., Lips P., van Schoor N.M., Vervloet M. G. Effect of 6-month Vitamin D supplementation on plasma matrix gla protein in older adults. Nutrients. 2019;11(2):231. doi:org/10.3390/nu11020231.
- Mager D. R., Qiao J., Turner J. Vitamin D and K status influences bone mineral density and bone accrual in children and adolescents with celiac disease. Eur J Clin Nutr. 2012;66(4):488-495. doi:org/10.1038/ejcn.2011.176.
- Jespersen T., Møllehave L. T., Thuesen B. H., Skaaby T., Rossing P., Toft U., Jørgensen NR, Corfixen B. L., Jakobsen J., Frimødt-Moller M., Linneberg A. Uncarboxylated matrix Gla-protein: A biomarker of Vitamin K status and cardiovascular risk. Clin Biochem. 2020;83:49-56. doi:org/10.1016/j.clinbiochem.2020.05.005.
- Roumeliotis S., Dounousi E., Eleftheriadis T., Liakopoulos V. Association of the inactive circulating matrix Gla protein with Vitamin K intake, calcification, mortality, and cardiovascular disease: A review. Int J Mol Sci. 2019;20(3):628. doi:org/10.3390/ijms20030628.
- Laurent S., Boutouyrie P., Asmar R., Gautier I., Laloux B., Guize L., Ducimetiere P., Benetos A. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension. 2001;37(5):1236-1241. https://doi.org/10.1161/01.HYP.37.5.1236.
- Schwalfenberg G. K. Vitamins K1 and K2: The emerging group of Vitamins required for human health. J Nutr Metab. 2017;6254836. doi:org/10.1155/2017/6254836.
- Simes D. C., Viegas C. S. B., Araújo N., Marreiros C. Vitamin K as a diet supplement with impact in human health: Current evidence in age-related diseases. Nutrients. 2020;12(1):138. doi:org/10.3390/nu12010138.
- Sozen T., Ozisik L., Basaran N. C. An overview and management of osteoporosis. Eur J Rheumatol. 2017;4(1):46-56. doi:org/10.5152/eurjrheum.2016.048.
- Shiraki M., Shiraki Y., Aoki C., Miura M. Vitamin K2 (menatetrenone) effectively prevents fractures and sustains lumbar bone mineral density in osteoporosis. J Bone Miner Res. 2000;15(3):515-521. doi:org/10.1359/jbmr.2000.15.3.515.
- Cancela L., Hsieh C. L., Francke U., Price P. A. Molecular structure, chromosome assignment, and promoter organization of the human matrix Gla protein gene. J Biol Chem. 1990;265(25):15040-15048. doi:org/10.1016/s0021-9258(18)77221-9.
- Poon C. C. W, Li R. W. S, Seto S. W, Kong S. K., Ho H. P., Hoi M. P. M., Lee S. M. Y., Ngai S. M., Chan S. W., Leung G. P. H. In vitro Vitamin K2 and 1α,25-dihydroxyVitamin D3 combination enhances osteoblasts anabolism of diabetic mice. Eur J Pharmacol. 2015;767:30-40. doi:org/10.1016/j.ejphar.2015.09.048.
- Van Ballegooijen A. J., Pilz S., Tomaschitz A., Grübler M. R., Verheyen N. The synergistic interplay between Vitamins D and K for bone and cardiovascular health: A narrative review. Int J Endocrinol. 2017;7454376. doi: 10.1155/2017/7454376.
- Manson J. A. E, Bassuk S. S., Buring J. E. Principal results of the Vitamin D and OmegA-3 TriaL (VITAL) and updated meta-analyses of relevant Vitamin D trials. J Steroid Biochem Mol Biol 2020;198:105522. doi:org/10.1016/j.jsbmb.2019.105522.
- Thakur M., Modi, V.K. Emerging Technologies in Food Science- focus on the developing world, Springer Nat 2020; 1- 287. doi.org/10.1007/978-981-15-2556-8.

This work is licensed under a Creative Commons Attribution 4.0 International License.






