
Introduction
With the change in people’s living habits and diet, the number of obese people is increasing year by year1. Obese people with large amounts of visceral adipose tissue are more likely to suffer from chronic diseases such as cardiovascular disease (CVD)2,3. Abdominal obesity, especially general obesity, presents a risk to both cardiovascular and cerebrovascular health 4-6. There are multiple approaches available for assessing obesity. Among these, the body mass index (BMI) is generally acknowledged to be the main and simple measure used in clinical environments. Nevertheless, BMI is impossible to differentiate between muscle mass and total body fat, and it does not effectively represent abdominal fat levels6-8. Consequently, various metrics for evaluating central obesity, including the lipid accumulation product (LAP), have been extensively utilized in clinical studies. The LAP is considered a trustworthy measure of visceral fat accumulation9,10. LAP, which serves as a measure for the overaccumulation of abdominal fat derived from triglycerides (TG) and waist circumference (WC), is regarded as the most reliable predictor of metabolic equivalence in individuals who are middle-aged and older11.
Nutrition, being a significant potential contributor of chemicals that are either pro- or anti-inflammatory, serves as a crucial regulator of inflammation12. After a thorough analysis of the body of research, the Dietary Inflammation Index (DII) can be used to assess the inflammatory effects of diet 13. To control the levels of six different inflammatory biomarkers—tumor necrosis factor-α(TNF-α), interleukin-4 (IL-4), C-reactive protein (CRP), interleukin 10 (IL-10), interleukin-1β (IL-1β), and interleukin-6 (IL-6)—a score was given to each of the 45 dietary factors14. DII value was negatively correlated with the anti-inflammatory ability of diet 15. DII combines the effects of all components on inflammation rather than depending on individual dietary assessments or recommended intake16,17. Diet is closely linked to disease and is easy to control and regulate, so choosing an anti-inflammatory diet may be an approach with high potential for beneficial effects. Investigation into the DII is quite comprehensive. For instance, research examining the links between DII and various chronic illnesses indicates that the possibility of food inflammation may increase the risk of chronic illnesses like diabetes, heart disease, depression, and cancer 18. Because chronic inflammation is significantly regulated by diet, a nutritious diet could help reduce the inflammatory response 19. Dietary interventions can serve to diminish both the prevalence and progression of inflammatory conditions, offering a cost-effective and accessible solution.
DII is an important tool for assessing the relationship between diet and health 20. Previous studies have provided preliminary evidence that there is a relationship between inflammation and LAP. The maintenance of lipid balance is intricately linked to the inflammatory immune response, with their cellular and molecular pathways interacting reciprocally21. Inflammation can induce podocyte lipid accumulation through dysregulation of the low-density lipoprotein receptor (LDLR) pathway22. Lipid peroxidation, insulin resistance, and systemic inflammation are significantly correlated with LAP in people with type 2 diabetes23. Given the limited previous research, a more complete understanding of the link between dietary inflammation and LAP is important for efficient prevention and treatment of central obesity. Surprisingly, there had been no previous reports of this particular relationship. To fill this gap, our study aims to explore the association between DII and LAP to provide important insights into how diet affects the pathophysiology of diseases such as central obesity, and ultimately to provide more theoretical support for the treatment and prevention of LAP-related diseases.
Materials and Methods
Data Sources
The National Health and Nutrition Examination Survey (NHANES) project conducts research on populations in different communities around the U.S. A sophisticated sampling design is used to randomly select people who are two months of age or older. The available data comprises structured questionnaires, physical examinations, laboratory results, and additional information. Data collection was reliably conducted and released every two years. The research acquired information from an ongoing cycle that extended from 1999 to 2018.
The research utilized published studies and collaborations that offer aggregate statistics that are accessible to the public. The studies were approved by an ethics review committee and individuals involved. Furthermore, this study did not employ individual-level data; hence, it is unnecessary to seek approval from a new ethics review committee.
Study Population
In the beginning, our analyses incorporated a total of 96,811 noninstitutionalized individuals. However, participants with absent LAP data (n=72,388) were removed from the study, along with those missing data for the DII (n=1,011). Furthermore, individuals who lacked other pertinent covariates were also excluded; this encompassed participants with absent data for variables, including marital status (n=919), education level (n=24), alcohol consumption (n=2,420), smoking status (n=13), hypertension (n=4), diabetes mellitus (n=576), chronic kidney disease (n=121), chronic obstructive pulmonary disease (n=1), cardiovascular disease (n=1), cancer (n=14), and poverty-to-income ratio (n=1,529). Ultimately, 17,790 participants participated (Figure 1).
 |
Figure 1: Flowchart of the study design and participants. |
DII Calculation
All participants in the NHANES trial were eligible to engage in two interviews centered on 24-hour dietary recalls. Interviews are conducted via mobile screening facilities and telephone. The dietary data used was based on the average compiled from both interviews.
DII was established by Shivappa via an exhaustive assessment of the available literature and was utilized13. The DII measures diet inflammatory potential by analyzing its association with six biomarkers and evaluates dietary intake for 45 nutrients. The global standard average method was used to calculate the Z-score for each participant. The z-scores were translated into proportions from 0 to 1, then centered by multiplying by two and subtracting one. The participants’ DII scores were calculated by taking into account the values of all dietary parameters. The dietary parameters include zinc, selenium, MUFA, protein, PUFA, and more.
LAP index calculation
The LAP index formula: [WC (cm) – 65] × [TG (mmol/l)] for males and [WC (cm) – 58] × [TG (mmol/l)] for females24-26.
Covariate Assessment
From the demographic survey, we collected information about participants’ demographics, which encompassed characteristics including age, gender, race, and educational attainment. The ethnic categories were listed in alphabetical order, comprising groups like Asian Americans, Native Americans, Latinos, and others. Options for marital status included living alone, marriage, or cohabitation. Participants were divided based on their poverty-to-income ratio (PIR), characterized as either below 2.5 or equal to or above 2.5, and categorized based on their educational attainment as individuals with less than a high school diploma, high school graduates, or holders of college degrees. The use of alcohol was categorized into five groups: former users, heavy users, mild users, moderate users, and non-users. Smoking behaviors were categorized as former smokers, non-smokers, or current smokers. Occurrences of diabetes mellitus (DM), as well as impaired fasting glucose (IFG) and impaired glucose tolerance (IGT), were documented.
Statistical Analysis
Data analysis was executed utilizing R software (version 4.2.3, R Foundation, http://www.R-project.org). The NHANES criteria were followed for weighing and evaluating the data. Constant variables are denoted as mean ± standard deviation (SD), whereas categorical data are conveyed in frequencies or percentages. This research employed linear regression to evaluate the impact of DII components on LAP. To reduce the impact of confounding variables on LAP and to discern the independent effect of DII, we conducted multiple regression analyses utilizing three distinct models. Model 1 was adjusted for ethnicity, age, and gender. Model 2 incorporated adjustments for PIR, educational attainment, marital status, alcohol intake, and tobacco use. Model 3 included all variables27-32. Furthermore, subgroup analyses classified participants based on age, gender, ethnicity, marital status, poverty income ratio, cancer history, chronic obstructive pulmonary disease, educational attainment, chronic kidney disease, cardiovascular conditions, diabetes mellitus, hypertension, smoking behaviors, and alcohol intake. This methodology sought to investigate whether the association between the DII with the LAP is stable across diverse subgroups and evaluate interactions among the relevant components. In accordance with the data distribution, the DII was classified as a binary variable to eliminate extreme values over 500 for the purpose of sensitivity analysis.
Results
Basic Characteristics
Information concerning the LAP and DII scores was obtained from 17,790 NHANES participants aged over 20 years. Table 1 summarizes the essential demographic characteristics and supplementary factors of individuals involved in the population of NHANES from 1999 to 2018, classified by DII score quartiles. The average age of participants in this specimen was 50.0 ± 17.8 years, with males comprising 50.9% of the total.
Table 1: The NHANES participants’ clinical and biochemical traits according to DII quartiles
|
Variables |
Total (n = 17790) | Q1 (n = 4448) | Q2 (n = 4447) | Q3 (n = 4447) | Q4 (n = 4448) |
P |
|
Age (years, mean± SD.) |
50.0 ± 17.8 | 49.6 ± 17.2 | 50.3 ± 17.6 | 49.8 ± 18.0 | 50.3 ± 18.4 | 0.147 |
| Sex, n (%) |
< 0.001 |
|||||
|
Female |
8743 (49.1) | 1609 (36.2) | 1986 (44.7) | 2383 (53.6) | 2765 (62.2) | |
| Male | 9047 (50.9) | 2839 (63.8) | 2461 (55.3) | 2064 (46.4) | 1683 (37.8) |
|
|
Race, n (%) |
< 0.001 | |||||
| Mexican American | 3069 (17.3) | 824 (18.5) | 803 (18.1) | 757 (17) | 685 (15.4) |
|
|
Non-Hispanic Black |
3421 (19.2) | 639 (14.4) | 776 (17.4) | 952 (21.4) | 1054 (23.7) | |
| Non-Hispanic White | 8497 (47.8) | 2239 (50.3) | 2143 (48.2) | 2075 (46.7) | 2040 (45.9) |
|
|
Other Race |
2803 (15.8) | 746 (16.8) | 725 (16.3) | 663 (14.9) | 669 (15) | |
| Marry, n (%) |
< 0.001 |
|||||
|
Living alone |
6856 (38.5) | 1494 (33.6) | 1580 (35.5) | 1820 (40.9) | 1962 (44.1) | |
| Married or living with a partner | 10934 (61.5) | 2954 (66.4) | 2867 (64.5) | 2627 (59.1) | 2486 (55.9) |
|
|
PIR, n (%) |
< 0.001 | |||||
| <2.5 | 9622 (54.1) | 2000 (45) | 2264 (50.9) | 2494 (56.1) | 2864 (64.4) |
|
|
≥2.5 |
8168 (45.9) | 2448 (55) | 2183 (49.1) | 1953 (43.9) | 1584 (35.6) | |
| Cancer, n (%) |
0.021 |
|||||
|
No |
16147 (90.8) | 4007 (90.1) | 4042 (90.9) | 4083 (91.8) | 4015 (90.3) | |
| Yes | 1643 (9.2) | 441 (9.9) | 405 (9.1) | 364 (8.2) | 433 (9.7) |
|
|
CVD, n (%) |
< 0.001 | |||||
| No | 15822 (88.9) | 4051 (91.1) | 3979 (89.5) | 3951 (88.8) | 3841 (86.4) |
|
|
Yes |
1968 (11.1) | 397 (8.9) | 468 (10.5) | 496 (11.2) | 607 (13.6) | |
| CKD, n (%) |
< 0.001 |
|||||
|
No |
14588 (82.0) | 3808 (85.6) | 3681 (82.8) | 3605 (81.1) | 3494 (78.6) | |
| Yes | 3202 (18.0) | 640 (14.4) | 766 (17.2) | 842 (18.9) | 954 (21.4) |
|
|
COPD, n (%) |
< 0.001 | |||||
| No | 17020 (95.7) | 4295 (96.6) | 4278 (96.2) | 4254 (95.7) | 4193 (94.3) |
|
|
Yes |
770 (4.3) | 153 (3.4) | 169 (3.8) | 193 (4.3) | 255 (5.7) | |
| Education, n (%) |
< 0.001 |
|||||
|
College |
9151 (51.4) | 2709 (60.9) | 2425 (54.5) | 2168 (48.8) | 1849 (41.6) | |
| High School or GED | 4132 (23.2) | 881 (19.8) | 969 (21.8) | 1078 (24.2) | 1204 (27.1) |
|
|
Less than high school |
4507 (25.3) | 858 (19.3) | 1053 (23.7) | 1201 (27) | 1395 (31.4) | |
| DM, n (%) |
< 0.001 |
|||||
|
DM |
3377 (19.0) | 716 (16.1) | 825 (18.6) | 886 (19.9) | 950 (21.4) | |
| IFG | 1658 (9.3) | 430 (9.7) | 439 (9.9) | 368 (8.3) | 421 (9.5) |
|
|
IGT |
1090 (6.1) | 274 (6.2) | 253 (5.7) | 264 (5.9) | 299 (6.7) | |
| No | 11665 (65.6) | 3028 (68.1) | 2930 (65.9) | 2929 (65.9) |
2778 (62.5) |
|
|
Hypertension, n (%) |
< 0.001 | |||||
| No | 10194 (57.3) | 2672 (60.1) | 2580 (58) | 2546 (57.3) |
2396 (53.9) |
|
|
Yes |
7596 (42.7) | 1776 (39.9) | 1867 (42) | 1901 (42.7) | 2052 (46.1) | |
| Smoke, n (%) |
< 0.001 |
|||||
|
Former |
4631 (26.0) | 1293 (29.1) | 1233 (27.7) | 1104 (24.8) | 1001 (22.5) | |
| Never | 9406 (52.9) | 2414 (54.3) | 2389 (53.7) | 2335 (52.5) | 2268 (51) |
|
|
Now |
3753 (21.1) | 741 (16.7) | 825 (18.6) | 1008 (22.7) | 1179 (26.5) | |
| Alcohol user, n (%) |
< 0.001 |
|||||
|
Former |
3148 (17.7) | 628 (14.1) | 702 (15.8) | 844 (19) | 974 (21.9) | |
| Heavy | 3537 (19.9) | 900 (20.2) | 901 (20.3) | 884 (19.9) | 852 (19.2) |
|
|
Mild |
6119 (34.4) | 1805 (40.6) | 1628 (36.6) | 1427 (32.1) | 1259 (28.3) | |
| Moderate | 2640 (14.8) | 645 (14.5) | 659 (14.8) | 701 (15.8) |
635 (14.3) |
|
|
Never |
2346 (13.2) | 470 (10.6) | 557 (12.5) | 591 (13.3) |
728 (16.4) |
|
Mean ± SD for continuous variables, % for categorical variables; PIR, Poverty-to-income ratio; DM, Diabetes mellitus; IFG, impaired fasting glucose; IGT, impaired glucose tolerance; CKD, Chronic kidney disease; LAP, Lipid Accumulation Products;COPD, Chronic obstructive pulmonary disease; CVD, Cardiovascular disease;
Association between DII with LAP
The relationship between DII with LAP is analyzed by linear regression method. Figure 2 presents a summary of the crude model alongside the adjusted models. Models 1 (β = 2.01, 95% CI = 1.40, 2.63, p < 0.001), 2 (β = 1.47, 95% CI = 0.83, 2.10, p < 0.001), and 3 (β = 0.86, 95% CI = 0.25, 1.47, p = 0.006) demonstrated a positive association between DII with LAP. Individuals involved were classified into quartiles according to their DII scores revealed that the third quartile exhibited a significantly higher LAP than the lowest quartile of DII. This was evident in model 1 (β = 8.28, 95% CI = 4.88, 11.67, p < 0.001), model 2 (β = 6.70, 95% CI = 3.43, 9.98, p < 0.001), and model 3 (β = 5.60, 95% CI = 2.41, 8.79, p < 0.001), as shown in Figure 2. The results showed that DII was positively correlated with LAP. Additionally, all p-values related to the trend test were significant in both the crude model and adjusted models 1 and 2.
 |
Figure 2: Multiple linear regression analysis on the association between DII and LAP in NHANES 1999–2018. |
Subgroup Analyses
Figure 3 illustrates the results derived from the subgroup analyses. Obvious, significant positive relationship was found amongst DII with LAP among male participants (β=1.41; 95% CI, 0.50, 2.31), those identified as Other Race (β=2.55; 95% CI, 1.06, 4.04), married individuals or those cohabiting with a partner (β=1.14; 95% CI, 0.38, 1.90), individuals with a PIR of 2.5 or higher (β=1.15; 95% CI, 0.28, 2.03), participants with No Cancer (β=0.85; 95% CI, 0.25, 1.45), those without CVD (β=1.02; 95% CI, 0.41, 1.63), individuals with No CKD (β=1.20; 95% CI, 0.55, 1.85), participants presenting No COPD (β=0.93; 95% CI, 0.32, 1.55), those who attended College (β=1.03; 95% CI, 0.18, 1.88), individuals with No DM (β=1.49; 95% CI, 0.87, 2.11), those exhibiting No Hypertension (β=1.54; 95% CI, 0.83, 2.24), never smokers (β=1.14; 95% CI, 0.38, 1.90), mild alcohol consumers (β=1.26; 95% CI, 0.35, 2.17), individuals involved under 60 years of age (β=1.04; 95% CI, 0.33, 1.76), and those who were 60 years or older (β=1.14; 95% CI, 0.07, 2.21). No other factors showed any association. Furthermore, the subgroup analysis indicated that DII did not interact with any of the subgroups.
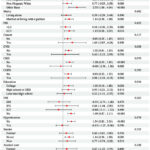 |
Figure 3: Subgroup analysis in NHANES 1999–2018. DM, Diabetes mellitus; CKD Chronic kidney disease; COPD Chronic obstructive pulmonary disease; CI, confidence interval. |
Sensitivity Analyses
We performed a sensitivity analysis that omitted participants with a DII greater than 500 anomalies, and the results of this evaluation were consistent with the initial analysis. In the sensitivity assessments, DII exhibited a positive correlation with LAP, irrespective of its classification as a continuous or categorical variable. The DII, when evaluated as an ongoing variable, correlated positively with LAP in a fully adjusted linear regression model (β: 1.02; 95% CI: 0.45, 1.60; p< 0.001). The third quartile of the DII (β: 4.04; 95% CI: 1.29-6.80; p=0.004) revealed a more robust association (Figure 4).
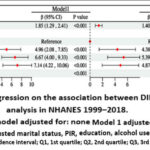 |
Figure 4: Multiple linear regression on the association between DII and LAP in the sensitivity analysis in NHANES 1999–2018. |
Discussion
Research has indicated that dietary habits can impact LAP and serve as a significant influencing factor for it33,34. Important insights were uncovered by this study that examined the eating patterns of adults in the US. Inflammation plays an important part in the connection between DII with LAP, which was uncovered by the research.
This study employs a cross-sectional design, we conducted an analysis of a sample of 17,790 participants. The relationship between DII with LAP in the original and adjusted models is proved by multivariate logistic regression data analysis. This indicates that DII and LAP are substantial correlations. This study establishes a solid foundation through the use of a thorough dataset and rigorous control measures, which makes the results more reliable and consistent.
Dyslipidemia is strongly associated with DII, and a pro-inflammatory diet may contribute to dyslipidemia and cardiovascular disease35. Studies have shown that plasma trans fatty acids can be used as a dietary inflammatory marker to predict heart disease 36. LAP is recognized as a novel biomarker linked to central lipid accumulation, which has the potential to predict the risk of diabetes and vascular abnormalities disease. Furthermore, it has demonstrated potential in forecasting NAFLD and metabolic syndrome. Research indicates that individuals with diabetes exhibit increased central lipid accumulation, which correlates with heightened insulin resistance, oxidative stress, and systemic inflammation9,23,37,38. The relationship between lipid homeostasis and inflammatory immune responses is intricate, with their cellular and molecular pathways influencing each other21. Circulating levels of proinflammatory cytokines are elevated in individuals with obesity. An increase in the mRNA expression and secretion of proinflammatory cytokines in the adipose tissue of obese individuals has been observed when examined in vitro39.
The majority of research endeavors have concentrated on elucidating the role of LAP in predicting various diseases. Investigations delving into the gender- and ethnicity-specific impacts of LAP have revealed its superior predictive capacity for insulin resistance risk among Asian males with normal blood glucose levels40. Our findings, which mirror significant results in the focused demographic groups, may be attributed to the higher prevalence of visceral fat in men41. The pertinent molecular biological mechanisms underlying these observations warrant further exploration. Regarding age-specific analyses, a previous study has indicated LAP as a potent predictor of metabolic syndrome in adolescents42. Our results also underscore more pronounced associations in age groups below 60 years. Intriguingly, our study hints at significant outcomes associated with higher levels of education, CVD, CKD, COPD, DM, hypertension, and non-smoking status. One plausible explanation could be that individuals with advanced educational backgrounds are more inclined to possess superior health education and adopt favorable lifestyle habits. Additionally, diabetes and hypertension are recognized as factors contributing to lipid accumulation43-45. Therefore, our findings may imply that inflammation linked to the DII might play a role in the development of LAP, although this hypothesis necessitates further validation through more extensive and comprehensive prospective studies.
This study’s advantage lies in the inclusion of the DII within the LAP study. DII, as a broad measure of diet-related inflammation in participants, facilitates a detailed analysis of the relationship between inflammatory dietary components and LAP. This integration enhances our understanding of how diet affects LAP, going beyond the usual focus on individual nutrients or categorized foods. In addition, an important feature of our study was to consider multiple variables to comprehensively assess the link between DII and LAP. Different dietary patterns play different roles in inflammation, and our study analyzed the effects of dietary factors on LAP outcomes through subtle differences.
There are some limitations to the tools used in the methodological aspects of this study. DII provides a comprehensive assessment of dietary inflammation, but many dietary components can affect DII46. Explaining the complexity involved in linking specific nutrient elements to the DII requires careful consideration. In addition, the 24-hour food recall method is a classic method, but it also has problems. A major concern is that it may not adequately capture typical dietary patterns due to changes in daily food intake. In addition, the accuracy of this method relies heavily on participants’ memory and recording of food consumption, which can lead to cases of underreporting or overreporting47,48. In response to these limitations, future research programs can provide a more comprehensive understanding through various food frequency questionnaires. Despite these challenges, the comprehensive data set in this study, the innovative introduction of DII, as well as scientific diet-related data collection methods substantially enrich this research. Our findings establish a basis for further research and potential nutritional treatments designed to manage or alleviate the dangers linked to LAP.
Conclusion
A positive correlation exists between DII with LAP, maintaining a lower inflammatory dietary pattern can help reduce the risk of adult obesity. Clear effects were observed in individuals who did not have CKD, DM, and hypertension. These breakthroughs have enabled effective screening and diagnosis of LAP. This research establishes the groundwork for future prospective investigations into the association between inflammation-inducing diets and NAFLD, metabolic syndrome, and diabetes. Dietary adjustment and its potential mechanism of action in inflammation and the formulation of dietary guidelines for the prevention of abnormal LAP in various populations are worthy of further study.
Acknowledgement
We would like to thank the public database NHANES for offering open-access, high-quality research resources.
Funding Sources
This study was supported by the National Natural Science Foundation of China (82200974).
Conflict of Interest
The authors do not have any conflict of interest.
Data Availability Statement
The manuscript incorporates all datasets produced or examined throughout this research study. Publicly available datasets were analyzed in this study. This data can be found at: https://www.cdc.gov/nchs/nhanes/.
Ethics Statement
The informed consent was obtained for experimentation in this study and it conforms to the standards currently applied in the U.S. The privacy rights of human subjects were observed. The National Center for Health Statistics in the United States gave its blessing to research projects that involved patients or other human beings. In order to participate in this study, each patient provided their written consent.
Informed Consent Statement
The informed consent was obtained for experimentation and that it conforms to the standards currently applied in the country of origin.
Permission to Reproduce Material from other Sources
Not applicable.
Clinical Trial Registration
This trial is registered at the NCHS Ethics Review Board (ERB) with the registration number: NCHS IRB/ERB Protocol #98-12; Protocol #2005-06; Protocol #2005-06; Protocol #2011-17; Continuation of Protocol #2011-17; Continuation of Protocol #2011-17; Protocol #2018-01 (Effective beginning October 26, 2017).
Author Contributions
- Yaxi Xu: Conceptualization, Methodology, Data Collection, Analysis, Writing-Original Draft.
- Ze Chen: Visualization, Supervision. Writing-Review & Editing.
- Chaoyong He: Writing-Review & Editing.
- Bin Wu: Visualization, Supervision. Writing-Review & Editing.
References
- Jaacks LM, Vandevijvere S, Pan A, et al. The obesity transition: stages of the global epidemic. Lancet Diabetes Endocrinol. Mar 2019;7(3):231-240. doi:10.1016/s2213-8587(19)30026-9
CrossRef - Haslam DW, James WP. Obesity. Lancet. Oct 1 2005;366(9492):1197-209. doi:10.1016/s0140-6736(05)67483-1
CrossRef - Pakhare M, Anjankar A. Critical Correlation Between Obesity and Cardiovascular Diseases and Recent Advancements in Obesity. Cureus. Jan 2024;16(1):e51681. doi:10.7759/cureus.51681
CrossRef - Bhupathiraju SN, Hu FB. Epidemiology of obesity and diabetes and their cardiovascular complications. Circulation research. 2016;118(11):1723-1735.
CrossRef - Kyrou I, Randeva HS, Tsigos C, Kaltsas G, Weickert MO. Clinical problems caused by obesity. 2015;
- Klein S, Allison DB, Heymsfield SB, et al. Waist circumference and cardiometabolic risk: a consensus statement from shaping America’s health: Association for Weight Management and Obesity Prevention; NAASO, the Obesity Society; the American Society for Nutrition; and the American Diabetes Association. Diabetes care. 2007;30(6):1647-1652.
CrossRef - consultation Obesity W. preventing and managing the global epidemic. Report of a WHO consultation. 2000.
- Franzosi MG. Should we continue to use BMI as a cardiovascular risk factor? The Lancet. 2006;368(9536):624-625.
CrossRef - Taverna MJ, Martínez-Larrad MT, Frechtel GD, Serrano-Ríos M. Lipid accumulation product: a powerful marker of metabolic syndrome in healthy population. European journal of endocrinology. 2011;164(4):559-567.
CrossRef - Amato MC, Giordano C, Galia M, et al. Visceral Adiposity Index: a reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes care. 2010;33(4):920-922.
CrossRef - Shin K-A, Kim Y-J. Usefulness of surrogate markers of body fat distribution for predicting metabolic syndrome in middle-aged and older Korean populations. Diabetes, metabolic syndrome and obesity: targets and therapy. 2019:2251-2259.
CrossRef - Galland L. Diet and inflammation. Nutr Clin Pract. Dec 2010;25(6):634-40. doi:10.1177/0884533610385703
CrossRef - Shivappa N, Steck SE, Hurley TG, Hussey JR, Hébert JR. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. Aug 2014;17(8):1689-96. doi:10.1017/s1368980013002115
CrossRef - Zhao S, Gao W, Li J, et al. Dietary inflammatory index and osteoporosis: the National Health and Nutrition Examination Survey, 2017-2018. Endocrine. Dec 2022;78(3):587-596. doi:10.1007/s12020-022-03178-6
CrossRef - Zhang C, Qiu S, Bian H, et al. Association between Dietary Inflammatory Index and kidney stones in US adults: data from the National Health and Nutrition Examination Survey (NHANES) 2007-2016. Public Health Nutr. Dec 2021;24(18):6113-6121. doi:10.1017/s1368980021000793
CrossRef - Shivappa N, Hébert JR, Rietzschel ER, et al. Associations between dietary inflammatory index and inflammatory markers in the Asklepios Study. Br J Nutr. Feb 28 2015;113(4):665-71. doi:10.1017/s000711451400395x
CrossRef - Bergmans RS, Malecki KM. The association of dietary inflammatory potential with depression and mental well-being among U.S. adults. Prev Med. Jun 2017;99:313-319. doi:10.1016/j.ypmed.2017.03.016
CrossRef - Park SY, Kang M, Wilkens LR, et al. The Dietary Inflammatory Index and All-Cause, Cardiovascular Disease, and Cancer Mortality in the Multiethnic Cohort Study. Nutrients. Dec 1 2018;10(12)doi:10.3390/nu10121844
CrossRef - Wirth MD, Shivappa N, Davis L, et al. Construct Validation of the Dietary Inflammatory Index among African Americans. J Nutr Health Aging. 2017;21(5):487-491. doi:10.1007/s12603-016-0775-1
CrossRef - Tan QQ, Du XY, Gao CL, Xu Y. Higher Dietary Inflammatory Index Scores Increase the Risk of Diabetes Mellitus: A Meta-Analysis and Systematic Review. Front Endocrinol (Lausanne). 2021;12:693144. doi:10.3389/fendo.2021.693144
CrossRef - Malekmohammad K, Bezsonov EE, Rafieian-Kopaei M. Role of Lipid Accumulation and Inflammation in Atherosclerosis: Focus on Molecular and Cellular Mechanisms. Review. Frontiers in Cardiovascular Medicine. 2021-September-06 2021;8doi:10.3389/fcvm.2021.707529
CrossRef - Zhang Y, Ma KL, Liu J, et al. Inflammatory stress exacerbates lipid accumulation and podocyte injuries in diabetic nephropathy. Acta Diabetologica. 2015/12/01 2015;52(6):1045-1056. doi:10.1007/s00592-015-0753-9
CrossRef - Mirmiran P, Bahadoran Z, Azizi F. Lipid accumulation product is associated with insulin resistance, lipid peroxidation, and systemic inflammation in type 2 diabetic patients. Endocrinol Metab (Seoul). Dec 29 2014;29(4):443-9. doi:10.3803/EnM.2014.29.4.443
CrossRef - Ahn N, Baumeister SE, Amann U, et al. Visceral adiposity index (VAI), lipid accumulation product (LAP), and product of triglycerides and glucose (TyG) to discriminate prediabetes and diabetes. Sci Rep. Jul 4 2019;9(1):9693. doi:10.1038/s41598-019-46187-8
CrossRef - Ebrahimi M, Seyedi SA, Nabipoorashrafi SA, et al. Lipid accumulation product (LAP) index for the diagnosis of nonalcoholic fatty liver disease (NAFLD): a systematic review and meta-analysis. Lipids Health Dis. Mar 15 2023;22(1):41. doi:10.1186/s12944-023-01802-6
CrossRef - Shi Y, Hu L, Li M, et al. Relationship Between the Lipid Accumulation Product Index and Arterial Stiffness in the Chinese Population With Hypertension: A Report From the China H-Type Hypertension Registry Study. Front Cardiovasc Med. 2021;8:760361. doi:10.3389/fcvm.2021.760361
CrossRef - Ding R, Han Z, Gui J, et al. Inflammatory properties of diet mediate the effect of epilepsy on moderate to severe depression: Results from NHANES 2013-2018. J Affect Disord. Jun 15 2023;331:175-183. doi:10.1016/j.jad.2023.03.054
CrossRef - Qu S, Fang J, Zhao S, et al. Associations of dietary inflammatory index with low estimated glomerular filtration rate, albuminuria and chronic kidney disease in U.S adults: Results from the NHANES 2011-2018. Nutr Metab Cardiovasc Dis. Apr 2024;34(4):1036-1045. doi:10.1016/j.numecd.2023.11.006
CrossRef - Zhou N, Xie ZP, Liu Q, et al. The dietary inflammatory index and its association with the prevalence of hypertension: A cross-sectional study. Front Immunol. 2022;13:1097228. doi:10.3389/fimmu.2022.1097228
CrossRef - Huang J, Han J, Rozi R, et al. Association between lipid accumulation products and osteoarthritis among adults in the United States: A cross-sectional study, NHANES 2017-2020. Prev Med. Mar 2024;180:107861. doi:10.1016/j.ypmed.2024.107861
CrossRef - Liu Q, Huang Y, Wang M, Jiang H, Zhang X. Association of lipid accumulation products with testosterone deficiency in adult American men: A cross-sectional study. Andrology. Mar 2023;11(3):551-560. doi:10.1111/andr.13355
CrossRef - Yan S, Chen S, Liu Y, et al. Associations of serum carotenoids with visceral adiposity index and lipid accumulation product: a cross-sectional study based on NHANES 2001-2006. Lipids Health Dis. Nov 30 2023;22(1):209. doi:10.1186/s12944-023-01945-6
CrossRef - Cicero AFG, D’Addato S, Reggi A, Reggiani GM, Borghi C. Hepatic Steatosis Index and Lipid Accumulation Product as middle-term predictors of incident metabolic syndrome in a large population sample: data from the Brisighella Heart Study. Internal and Emergency Medicine. 2013/04/01 2013;8(3):265-267. doi:10.1007/s11739-012-0875-9
CrossRef - Seong JM, Lee JH, Gi MY, et al. Gender difference in the association of chronic kidney disease with visceral adiposity index and lipid accumulation product index in Korean adults: Korean National Health and Nutrition Examination Survey. International Urology and Nephrology. 2021/07/01 2021;53(7):1417-1425. doi:10.1007/s11255-020-02735-0
CrossRef - Chen X, Hou C, Yao L, et al. Dietary inflammation index is associated with dyslipidemia: evidence from national health and nutrition examination survey, 1999–2019. Lipids in Health and Disease. 2023/09/09 2023;22(1):149. doi:10.1186/s12944-023-01914-z
CrossRef - Mazidi M, Gao H-k, Shivappa N, Wirth MD, Hebert JR, Kengne AP. The relationship of plasma Trans fatty acids with dietary inflammatory index among US adults. Lipids in Health and Disease. 2017/08/04 2017;16(1):147. doi:10.1186/s12944-017-0527-1
CrossRef - Dai H, Wang W, Chen R, Chen Z, Lu Y, Yuan H. Lipid accumulation product is a powerful tool to predict non-alcoholic fatty liver disease in Chinese adults. Nutrition & Metabolism. 2017/08/01 2017;14(1):49. doi:10.1186/s12986-017-0206-2
CrossRef - Ebrahimi M, Seyedi SA, Nabipoorashrafi SA, et al. Lipid accumulation product (LAP) index for the diagnosis of nonalcoholic fatty liver disease (NAFLD): a systematic review and meta-analysis. Lipids in Health and Disease. 2023/03/15 2023;22(1):41. doi:10.1186/s12944-023-01802-6
CrossRef - Coppack SW. Pro-inflammatory cytokines and adipose tissue. Proc Nutr Soc. Aug 2001;60(3):349-56. doi:10.1079/pns2001110
CrossRef - Shajith Anoop S, Riddhi D, Grace R, et al. Lipid accumulation product (LAP) as a potential index to predict risk of insulin resistance in young, non-obese Asian Indian males from Southern India: observations from hyperinsulinemic-euglycemic clamp studies. BMJ Open Diabetes Research & Care. 2021;9(1):e002414. doi:10.1136/bmjdrc-2021-002414
CrossRef - Karpe F, Pinnick KE. Biology of upper-body and lower-body adipose tissue–link to whole-body phenotypes. Nat Rev Endocrinol. Feb 2015;11(2):90-100. doi:10.1038/nrendo.2014.185
CrossRef - Chen Z-y, Liu L, Zhuang X-x, et al. Lipid accumulation product is a better predictor of metabolic syndrome in Chinese adolescents: a cross-sectional study. Original Research. Frontiers in Endocrinology. 2023;14
CrossRef - Khanmohammadi S, Tavolinejad H, Aminorroaya A, Rezaie Y, Ashraf H, Vasheghani-Farahani A. Association of lipid accumulation product with type 2 diabetes mellitus, hypertension, and mortality: a systematic review and meta-analysis. Journal of Diabetes & Metabolic Disorders. 2022/12/01 2022;21(2):1943-1973. doi:10.1007/s40200-022-01114-z
CrossRef - Agata J, Miyazaki Y, Takada M, et al. Association of insulin resistance and hyperinsulinemia with disturbed lipid metabolism in patients with essential hypertension. Hypertens Res. Mar 1998;21(1):57-62. doi:10.1291/hypres.21.57
CrossRef - Petrie JR, Guzik TJ, Touyz RM. Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mechanisms. Canadian Journal of Cardiology. 2018/05/01/ 2018;34(5):575-584. doi:https://doi.org/10.1016/j.cjca.2017.12.005
CrossRef - Xie R, Ning Z, Xiao M, Li L, Liu M, Zhang Y. Dietary inflammatory potential and biological aging among US adults: a population-based study. Aging clinical and experimental research. 2023;35(6):1273-1281.
CrossRef - Xie R, Zhang Y. Association between 19 dietary fatty acids intake and rheumatoid arthritis: results of a nationwide survey. Prostaglandins, Leukotrienes and Essential Fatty Acids. 2023;188:102530.
CrossRef - Xie R, Zhang Y. Associations between dietary flavonoid intake with hepatic steatosis and fibrosis quantified by VCTE: Evidence from NHANES and FNDDS. Nutr Metab Cardiovasc Dis. Jun 2023;33(6):1179-1189. doi:10.1016/j.numecd.2023.03.005
CrossRef

This work is licensed under a Creative Commons Attribution 4.0 International License.






