
Introduction
Alkaline phosphatases (ALP) are the metalloenzymes of cell membrane and they are synthesised in intestines, liver, bone, placenta and in the proximal convoluted tubules of kidney.1,2 The serum ALP activity is primarily from the liver and 50% given by bone3 Tumor specific isoenzymes of ALP such as Nago, Regan and Kasahara are secreted by tumors into plasma.4 These enzymes act upon in alkaline pH (pH≥ 10) and are dormant in the blood. The exact metabolic functions of the enzyme is not so far understood. It emerges that ALP is linked with calcification process in bone and with lipid transport in intestine. It catalyses hydrolysis of phosphate esters in an alkaline environment, generating an organic radical and inorganic phosphate from molecules like nucleotides, proteins and alkaloids1 ALP exists in numerous forms, some of which are true isoenzymes, encoded at different genetic loci.5
Serum ALP activity is usually measured to detect increases in its activity. Increased activity of ALP occurs in pregnancy, childhood, paget’s disease, intra and extrahepatic cholestatis and various other bone diseases. ALP level are highest in the first 6 months of life, reduce to reasonably steady levels subsequently and starts to raise after 9 years due to increased osteoblastic activity. It declines toadult range after 20 yrs of age in boys and 17-18 yrs in girls.6,7
Very less attention has been focused on clinical conditions associated with low or decrease ALP activity in humans. Various causes may attribute to low ALP activity such as hypophosphatasia, cardiac surgery and cardiopulmonary bypass, blood collected with EDTA or oxalate anticoagulant, hypothyroidism, vitamin C and B12 deficiency, Milk alkali syndrome, protein/ calorie malnutrition, zinc and magnesium deficiency.8,9
Divalent ions such as Mg2+, Co2+& Mn2+ are activators of the ALP and Zn2+ is a constituent metal ion. The accurate ratio of Mg2+/ Zn2+ ions is necessary to avoid displacement of Mg2+ and to obtain optimal activity.3 Low dietary Magnesium has been associated with low ALP activity and rats fed with Mg deficient diet demonstrated depressed ALP activity that was reversed by adding Mg in their diet.10 Many studies have also shown that Zn deficiency depressingly affects bone related enzymes and minerals such as ALP and Ca, P and Mg.2
With the above observations, our study is aimed to establish the prevalence of mineral deficiency in people with low ALP activity and during routine check up for LFT estimation, the extent of mineral deficiency in various social groups can be obtained.
Materials and Methods
This cross sectional study was conducted in Dept. of Biochemistry, Institute of Medical Sciences, Bhubaneswar under the aegis of Siksha ‘O’ Anusandhan University. The study includes Outpatients and Inpatients of the hospitals within the age group of 20-50 years. The subjects are selected from the patients who give blood for estimation of liver function test (LFT) for any reason.
Detailed history is taken from them and ALP activity in their serum is measured by Roche Cobas Integra 400 plus auto analyzer using International Federation of Clinical Chemistry (IFCC) Gen-2 method.11 An ALP value of 45-115 Units/Liter (U/L) in an adult population is considered normal.2 The study group includes 42 subjects with low ALP activity (<45 U/L) as cases and 45 age and sex matched healthy controls with normal ALP as control population. Blood from these persons are subjected to Zn and Mg estimation.
Serum Zn is estimated by 2-(5-Nitro-2-pyridylazo)-5-(N-n-propyl-N-(3-sulfopropyl)amino)phenol, disodium salt, dehydrate (Nitro-PAPs) method and serum Mg is determined by Calmagite method in semi autoanalyzer (Photometer 5010) using commercially available kits.12,13
Causes of low Zn level such as cirrhosis, lung cancer, Acute Myocardial Infarction (AMI), renal failure, sickle cell anemia, corticosteroids and oral contraceptive therapy and causes of decrease level of Mg such as malabsorption, treatment phase of Diabetic coma, chronic renal disease, chronic alcoholism, pancreatitis and hyperthyroidism are also excluded from the study group.
The data were analysed with SPSS 20.0 software. Continuous data were expressed in terms of mean and standard deviation and proportions in terms of percentages. Means were compared using students’t-test. Correlation between continuous variables was done using pearson’s correlation test. We consider a p value of <0.05 as statistically significant.
The study was approved by the institutional ethical committee. An informed written consent was obtained prior to the study seeking permission to participate in the study.
Results and Discussion
A total of 42 cases and 45 controls within the age group of 20-50yrs were included in the study group.
Table-1 shows 20 out of 42 cases were Zn deficient, taking 60-120 µg/dl as the normal range. Zn deficiency in control groups was found to be 3 among 45 persons. It has been observed that 22 out of 42 cases were Mg deficient, taking 1.3-2.5mEq/L as the normal range. Mg deficiency in control groups was found to be 3 out of 45 persons.
When Zn and Mg values were estimated in the study group, mean Zn values in cases was found to be 59.21±17.1 µg/dl in comparison to 73.4±8.6 µg/dl in controls which was statistically significant. Similarly mean Mg value was 1.26±0.37 mEq/L in cases and 1.8±0.56 mEq/L in controls which was also statistically significant (Table-2).
Table 1: Percentage of Zn and Mg deficiency in study population
| Controls | Cases | |||||
| Zn deficient | Mg deficient | total | Zn deficient | Mg deficient | total | |
| Number | 3 | 6 | 45 | 20 | 22 | 42 |
| Percentage | 6.67 | 13.34 | 100 | 47.62 | 52.38 | 100 |
Table 2: Mineral levels in the study group
| Parameters | Control (n=45) | Cases (n=42) | p value |
| Zn (µg/dl) | 73.4±8.6 | 59.21±17.1 | <0.001 |
| Mg (mEq/L) | 1.8±0.56 | 1.26±0.37 | <0.05 |
Correlation between Zinc and alkaline phosphatase (r=0.553, p<0.001) was found to be statistically significant (Fig-1). When values of Mg were correlated with alkaline phosphatase values using Pearson’s correlation, r value was 0.491 and it was statistically significant with the p value <0.05 ( Fig-2).
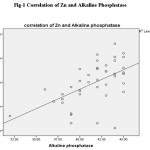 |
Figure 1: Correlation of Zn and Alkaline Phosphatase Click here to View figure |
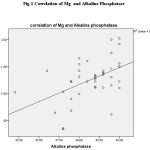 |
Figure 1: Correlation of Mg and Alkaline Phosphatase Click here to View figure |
ALP enzyme has important investigative role to play in liver diseases and bone diseases. It has important role in differentiating parenchymal liver diseases to obstructive liver diseases. The decrease in ALP is also found to have diagnostic role in detecting various diseases. Our study includes the patients within 20-50 yrs of age group. This excludes children having cretinism and achondroplasia and postmenopausal women having osteoporosis.
It was found out that 17 out of 42 cases were females suggesting the fact that low ALP is common in female population.10
We found a significant decrease in Zn and Mg level in our group of cases suggesting the fact that, ALP is a Zn containing metalloenzyme and Mg is an important promoter of ALP which is in concurrence with the authors Naber, et al and Arise, et al.,14,15
In this study 52.38% of cases are Magnesium deficient, whereas 47.62% of cases are Zn deficient which is higher than the percentage found by other authors.10
There is a positive correlation between Zn and Alkaline phosphatase in these groups signifying the fact that Zn raises the activities of alkaline phosphatases particularly of bone. It also activates osteoblast tyrosine kinase and RNA synthetase suggesting its role in bone formation. This is in concordance with Peretz, et al., and Yamaguchi, et al.,16,17 The present study reveals a significant positive correlation between Mg and ALP which suggests the fact that divalent metal ion Mg is a potent stimulator of ALP. Mg occupies the structural site on ALP to convert it to a more active form.15 Femi J Olorunniji, et al in their study showed that Mg and Zn ions interact to activate the non specific tissue alkaline phosphatase.18 Metal ions participate in catalysis, stabilisation of protein structure and regulation of activities of metalloenzymes. The definite binding of Mg to apo-ALP depends on both the cooperative effects of Zn binding and pH. Mg regulates the Zn induced restoration of activity and structural integrity of metal binding loci.18
Conversely studies by other authors have shown a decrease in ALP activity in the haemolysed sample having high Zn and Mg levels. This could be due to the fact that Zn and Mg exert feedback inhibition on ALP activity.19 Lum, et al., also found other important causes of decrease ALP activities of which cardiac surgery, malnutrition, hypophosphatasia, hypothyroidism, vitamin B12 deficiency are important.19 We have not considered these criteria into account in this study.
Our study reveals a strong association of Zn and Mg levels with ALP activity. Hence Zn and Mg supplementation can increase the alkaline phosphatase level in deficient groups.
Conclusion
It was concluded that ALP activity is not only important for increase in its activity, but it is also important for decrease in its activity. Zn and Mg deficiency are the most important causes of low ALP activity. Thus this research establishes the prevalence of mineral deficiency in people with low ALP activity. During usual check up for Liver function test, the degree of mineral deficiency in different social groups can be obtained. Since Zn & Mg are essential for bone growth, remodelling and various other metabolism in the body, their replacement in the diet can be set off. The diet containing phosphorus, healthy fats, Zn, vitamin B12 and vitamin A can be started to increase alkaline phosphatase level.
Acknowledgements
We would like to thank Mr.Abhijeet Senapati for his contribution.
References
- Warnes TW. Alkaline phosphatase. Gut. 1972;13(11):926–937.
CrossRef - Young-Eun Cho, Ria-Ann R. Lomeda, Sang-HoonRyu, Ho-Yong Sohn, Hong-I Shin and John H. Beattie, et al. Zn deficiency negatively affects alkaline phosphatase and the concentration of Ca, Mg and P in rats. Nutrition Research and Practice. 2007;2:113-119.
- Tietz textbook of Clinical Chemistry and Molecular Diagnostics, Burtis C.A.; 4th Edition: 608-612.
- Rosalki SB and Mcintyre N. Biochemical investigations in the management of liver disease; Oxford textbook of clinical hepatology, 2nd ed. New York: Oxford university press. 1999;503–521.
- Moss DW. Perspectives in Alkaline phosphatase research. Chem. 1992;38:2486-92.
- Schiele F, Henny J and Hitz J. Total bone and liver alkaline phosphatase in plasma: biological variations and reference limits. Chem. 1983;29:634–641.
- Turan S, Topcu B, Gokce I, Guran T, Atay Z, Omar A, Akcay T and Bereket A. Serum alkaline phosphatase levels in healthy children and evaluation of alkaline phosphatase z-scores in different types of rickets. Clin. Res. Pediatr. Endocrinol. 2011;3(1):7–11:.
CrossRef - Simko V. Alkaline phosphatases in biology and medicine. Dis. 1991;9:189–193.
CrossRef - Lum G. Significance of Low Serum Alkaline Phosphatase activity in a predominantly adult male population. Chem. 1995;41(4):515-518.
- Pimstone B, Eisenberg E and Stallone W. Decrease in Serum alkaline phosphatase activity produced by magnesium depletion in rats. Soc.Exp.Biol.; Med. 1966;123:201-3.
CrossRef - Tietz NW et al. Clin.Chem.Clin.Biochem. 1983;21:731-740.
- Tetsuo Makino. Chem.Acta. 1991;197:209-220.
CrossRef - Clinical Chemistry, Principles, Procedures, Correlations, Michael L.Bishop, et al; 5th
- Naber THJ, Baadenhuysen H, Jansen JBMJ, van den Hamer C and van den BroekNR. Serum alkaline phosphatase activity during zinc deficiency and long-term inflammatory stress. Chim.Acta. 1996;249:109–127.
CrossRef - Arise R. O., Davies F. F. and Malomo S. O. Independent and interactive effect of Mg2+ and Co2+ on some kinetic parameters of rat kidney alkaline phosphatase. Res. Ess. 2008;3:488–494.
- Peretz A, Papadopoulos T, Willems D, Hotimsky A, Michiels N, Siderova V, Bergmann P and Neve J. Zinc supplementation increases bone alkaline phosphatase in healthy men. Trace Elem. Med. Biol. 2001;15:175–178.
CrossRef - Yamaguchi M and Inamoto K. Differential effects of calcium-regulating hormones on bone metabolism in weanling rats orally administered zinc sulfate. Metabolism. 1986;35:1044–1047.
CrossRef - Olorunniji FJ, Igunnu A, Adebayo JO, Arise RO and Malomo SO. Cofactor interaction in the activation of tissue non-specific Alkaline phosphatase: Synergistic effects of Zn2+ and Mg2+ Biokemistri. 2007;19:43–48.
- Farah, H, Al-Atoom, A and Shehab, G. Explanation of the decrease in alkaline phosphatase (ALKP) activity in hemolyzed blood samples from the clinical point of view: in vitro study. Jordan J. BiolSci. 2012;5:125–128.

This work is licensed under a Creative Commons Attribution 4.0 International License.







