
Introduction
Inflammatory diseases of oral cavities and soft tissue changes are associated with diabetes mellitus.1 Taste disorder is a common observation in type 1 and type 2 diabetes . The threshold for bitter taste is reduced in these patients due to diabetic neuropathy. It is reported that more than 250 medications affect smell and taste sensation in diabetes.2 Dietary intervention plays a major role in the treatment of type II diabetes along with drugs and exercise. Low carbohydrate diet (30-40%) followed for more than hundreds of years is no longer necessary. It is universally agreed that carbohydrate may form 60-65% of total calories .Three fourth of total carbohydrate may come preferably from complex carbohydrate like unrefined cereals in the form of hand pounded rice, whole wheat, ragi and cumbu.3 The gluten present in wheat increases the chewing counts and the sense of satiety. The dietary fiber present in milled cereals increases the standing time of food in the gut and fullness to prevent hyperglycemia. An optimum level of fiber would be 25gms per 1000 calories . Green leafy vegetables like cluster beans, kovakkai, plantain stem and ladies finger are rich sources of dietary fiber. In the management of hyperlipedemia in obese T2dm fat content should be reduced to 20-25%. The unsaturated fatty acid(UFA) present in olive oil, cottonseed oil, corn oil, soy bean oil and sunflower oil, are necessary for the metabolism and function.4 There is evidence that T2dm can be treated by the use of indigenous foods like bitter gourd juice, ginger, garlic oil, thulasi extract, jamun seed extract and fenugreek seeds.5 Fenugreek (Trigonella foenum graecum) is a common condiment used in Indian homes as a spice and food to reduce hyperglycemia.6 About 25-100gms of fenugreek seeds taken daily can diminish reactive hyperglycemia. The beneficial effect of soluble dietary fiber fraction of fenugreek on insulinemic and lipidimic status in type 2 diabetes is well established.7 Indian diet recipes and food ingredients are yet to be standardized. In a heterogeneous culture like ours one has to necessarily take into account the factors such as regional and local food habits, cooking habits, eating habits, timing and frequency of food intake, various recipes, and indigenous dietetic ideas prevalent in the society.8 Sensory analysis of a product is related to the organoleptic feel of the product. They are the visible attributes like appearance and color.The tactile feel consists of texture and the olfactory and gustatory sensation are the flavor per se and taste per se.9
Materials and method
The study was approved by the research committee of Sri Avinashilingam deemed university and designed to include eligible T2DM and normoglycaemic individuals A written consent was obtained and were appraised of the study. The ingredients for recipe standardization was procured from chintamani supermarket (Coimbatore).
Sample size
Purposive sampling procedure was followed. Eligible 20T2DM taking oral hypoglycaemic drugs(Past2-3years) and 20 normoglycaemic individuals in the age group of 35-45 years from among the staff members comprised the study.
Product development
Idea generation and screening of ideas were the initial step in product(dhokla) development using food-to- food fortification strategy. The fenugreek seeds were treated to remove lectins, debitterized and processed fenugreek powder was used to remove undesirable taste.10
Fenugreek seeds (purchased in lots)
↓
Soaked (hot boiling water- 1 minute )
↓
Inactivate lectins (To ↓ fenugreek odour)
Seeds Dried (Evaporation)
↓
To remove moisture
Fried slightly
↓
To remove the bitterness
Powdered (Flour mill)
↓
To pass through a 60’ mesh sieve
Treated Fenugreek Flour
( Packed blends of 10,15 ,20 and 25per cent )
After a series of trials using ingredients in various proportion(Table-1) the concept of the enriched product-dhokla took shape. Dhoklas the indian recipe was selected for fortification with treated fenugreek flour due to its commonality of use in Indian homes. The recipe had four variation with four blends (10 per cent, 15 per cent,20 per cent and 25 per cent) with a control. The recipes were standardized in the food science laboratory for its repeated.
Table 1: Ingredients in dhokla preparation
|
S.no |
Ingredients |
Amount |
|
1 |
Maize flour |
100 gms |
|
2. |
.Wheat flour |
10 gms |
|
3. |
Onions |
20 gms |
|
4 |
Chillies |
2 gms |
|
5 |
Oil |
10 ml |
|
6 |
Fenugreek |
15gms |
|
7 |
Salt |
pinch |
|
8 |
Water |
30 ml |
100gms contains 20gms fenugreek flour
100gms yield 5 dhoklas
consistency . Score cards were developed as given in table 1 using product related lexicon based on 5 point hedonic scale rating . One recipe with four variation was prepared .The recipes were coded as S1 , S2 , S3 and S4 to prevent any bias. The panel members were invited by 12.30 pm for sensory analysis. A glass of water was provided to rinse their mouth each time they tasted a different variation.
Table 1a: Score card to evaluate dhoklas
| Appearance | Colour | Texture | Flavour | Taste | Score |
| a. Very Good | a. Golden Yellow | a. Soft | a. Highly Acceptable | a. Good | 5 |
| b. Good | b. Yellow | b. ModeratelySoft | b. Acceptable | b. Fair | 4 |
| c. Fair | c. Light Yellow | c. Fairly Hard | c. Mild FenugreekFlavour | c. Slightly Bitter | 3 |
| d. Poor | d. Yellowish Brown | d. Soggy | c. Strong FenugreekFlavour | d. Bitter | 2 |
| e. Very Poor | e. Brown | e. Hard | e. Raw Flavour | e. Highly Bitter | 1 |
Statistical Analysis
The results were statistically analyzed using 2- way anova with interaction and post-hoc test for paired comparison.
Results
Table 3 shows that there was significant difference ( P<0.001) in rating of dhoklas by diabetics and normoglycaemics at 20 and 25 per cent of fenugreek incorporation. Pathological changes in the peripheral nerves of diabetics affects the myelin sheath resulting in reduced thresh hold for bitter taste.11 A significant difference(P<0.001) in perception of different attributes was observed at 15, 20 and 25 per cent. An altered sensitivity to various perceptions was seen in diabetics. Continuously a significant difference( P<0.001) in interaction was observed at 25 per cent between experimental and control group for perception of different attributes. Lectins present in fenugreek is the cause for its odour.12 They were removed by soaking with-out compromising the taste and flavor.
Table 2: Organoleptic evaluation of dhoklas as rated by diabetics and normoglycaemics
| Variation | Diabetic | Normoglycaemic | P-Value | ||||||||||
| Apperance | Colour | Texture | Flavour | Taste | Apperance | Colour | Texture | Flavour | Taste | Patients | Characters | P×CI | |
| 10 percent S1 | 4±0.25a | 4±0.25a | 4.6±0.11a | 3.7±0.18ab | 4.2±0.17a | 3.7±0.18ab | 4±0.23a | 4±0.18a | 3.8±0.2ab | 3±0.23b | o.oo3 | 0.01 | 0.008 |
| 15per cent S2 | 3.7±0.18bc | 3.8±0.2ab | 4.6±0.11a | 3.4±0.18bc | 3.8±0.2ab | 3.6±0.15bc | 3.8±0.2ab | 3.8±0.2ab | 3.4±0.18bc | 3.0±0.23c | 0.004 | <0.001 | 0.036 |
| 20PercentS3 | 3.2±0.22bc | 3.8±0.2ab | 4.4±0.11a | 3.0±0.23c | 3.8±0.2ab | 3.4±0.18bc | 3.4±0.18bc | 3.8±0.2ab | 2.8±0.092c | 2.8±0.092c | <0.001 | <0.001 | 0.015 |
| 25PercentS4 | 3.2±0.22bc | 3.7±0.18ab | 4.2±0.17a | 2.8±0.092c | 3.7±0.18ab | 3.4±0.18bc | 3.4±0.18bc | 3.4±0.18bc | 2.8±0.092c | 2±0.018d | <0.001 | <0.001 | <0.001 |
Values are means ±SEM,n =20 per treatment group.
Means in a row without a common superscript letter differ( <0.005) as analysed by two-way anova.
P×CI = Patients ×Characters interaction effect
Results of post-hoc tukey test revealed that there was significant difference (P<0.005) in taste perception between experimental and control group at all four levels of fenugreek incorporation
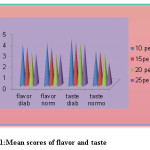 |
Figure 1: Mean scores of flavor and taste Click here to View figure |
The diabetic mean score (4.2±0.17) was higher than normoglycaemics (3 ± 0.23) at 10 per cent. Diabetic neuropathy has possibility to change all four senses of taste. Continuously a higher mean score was marked by diabetics stating that the taste acquity for bitterness was lesser in diabetics than normoglycaemics.13 At 25 per cent level of fenugreek incorporation again diabetics scored maximum(3.7±0.18) compared to normoglycaemics (2 ±0.18).Acceptability of food products in terms of sensory variables is an important step in determining research priority.14 The perception to bitter flavor was reduced in diabetics with a highest (3.0.23) mean score compared to normoglycaemics (2.8±0.09) at 15 per cent.
In determining the sensitivity to bitter flavor and taste perception in diabetics a significant difference (P<0.005) was seen at different levels of fenugreek incorporation. The diabetics had low threshold for bitter flavor and scored a maximum (3.7±0.17) at 10 per cent. The bitterness was not felt until 20 per cent. The threshold for bitterness was perceived at 25 percent with a minimum(2.8±0.09) score. Systemic disorders like diabetes mellitus can secondarily cause taste changes through neuropathy.15 In terms of taste perception again the threshold was decreased with a maximum score (4.2±0.17) at 10 per cent. A higher thresh hold for bitter taste was perceived at 25 per cent with a (3.7±0.17) minimum score. Sensory analysis techniques have been developed into powerful tool for understanding how sensory attributes emphasize product quality and consumer preferences. Modern techniques of sensory processing can be very useful for optimizing, new product.16
 |
Figure 2: Dhoklas with variation in fenugreek flour Click here to View figure |
The dhoklas had a high level of acceptability (fig -2) at 10 per cent of fenugreek incorporation in terms of appearance (4±0.25), colour(4±0.25) and texture (4.6±0.17).The product was less acceptable at 20 and 25 per cent with the lowest mean score.
Discussion
Fenugreek was found bitter in taste but incorporating treated fenugreek flour in recipes in varied concentration decreased the bitterness. The diabetics have decreased taste sensitivity for all taste parameters i.e. sweet, salt, sour and bitter.17 A significant difference (P<0.001) at 20 and 25 per cent was found between diabetics and normoglycaemics. The post-hoc test reveals significant difference ( P<0.005) in taste perception between diabetics and normoglycaemics at all four levels. The flavor perception also differed significantly (P<0.005) between various concentration in diabetics. The threshold for bitter taste was perceived slightly at 25 per cent level in diabetics. The product was acceptable at 10 per cent.
Conclusion
The study revealed a lower sensitivity to bitter flavor and taste modality in diabetics. The threshold for bitter taste was perceived only at higher concentration of 25 percent in, dhoklas. Treated fenugreek flour can be incorporated to about 25 per cent to reduce blood sugar in type II diabetes due to its higher threshold for bitter sensitivity.
Acknowledgements
The author wishes to acknowledge the staff members of Avinashilingam University for their support as being the members of taste panel.
References
- Shailesh M. G, Atul I, Shirish D, Rahul B. Evaluation of gustatory function in patients with diabetes mellitus type 2. Oral Surgery, Oral Medicine, Oral Pathology and oral Radiology. 2009;108(6).
- Shanaz Mohammad Gaphor, Raz A. Saeed. The evaluation of taste threshold for four main tastes between diabetic and healthy individuals. European Scientific Journal. 2014;10(3):435-439.
- Viswanathan M, Ramachandran A, Mohan V, Snehalatha C, Dietary management of diabetes mellitus an update, Diet, digestion and diabetes. Workshop manual, 10. 4. diabetes association of india. 1983:82(2)206.
- Viswanathan M, Ramachandran A , Indira P, Sherry J, Snehalatha C, Mohan V , Kymal PK. Responses to legumes in NIDDM subjects: lower plasma glucose and higher insulin levels. Nutritional Reports International. 1989;40:803-812.
- Kashikar v.s, kotkar Tejaswita. Indigenous remedies for diabetes mellitus, Int J Pharm PharmSci.2011;3(3):22-29.
- Giri J, Sakthidevi T.K, Meerarani S, The effect of ginger on serum cholesterol and blood glucose levels. Society of biological chemists,abstract; Baroda. 85.
- Nutrition News, Use of fenugreek seeds (Trigonella foenum graecum) by diabetics, . Nutrition News ;National Institute of Nurition, ICMR. 1987;8(4).
- Munichoodappa C,Lalitha C.K, Indigenous dietetic ideas in diabetic dietetic regiment, Diet, Diabetes and Digestion, Workshop manual, 10. 4. diabetes association of india. 1983;82(2)206.
- Paul P.C, Palmer H.H, Sensory methods of food quality assessment, Food theory and applications;John wiley and sons. 1972;727.
- Paturi V Rao, Use of Plant Foods including Bitter Gourd and Fenugreek in managing type 2 diabetes mellitus, International Journal of Diabetes in Developing Countries;9: October 1989.
- Olson R.K, Taste changes in diabetes mellitus. Nutrition review. 1982;40(8):236-237.13.
- Hypoglycaemic effect of fenugreek; Annual report National institute of nutrition ICMR. 1984-198585;11.
- Sudharshani W, Priyadarshika H, Shamini P, Sweet taste sensitivity in pre-diabetics,diabetics and normoglycaemic controls: a comparative cross sectional study, BMC Endocrine disorders. 2014;14:67.
CrossRef - Morr M.L,Irmiter T.F, Evaluation of food products, Introductory foods, II Edition,Macmillan publishing company. 1975;446.
- Hardy S.L, Brennand C.P. Taste threshold of individuals with diabetes mellitus and of control subject. Journal of American dietetic association. 1988;79(3):286-289.
- Crina Muresan, Laura Stan, Simona Man, Stancuta Scrob, Sevastita Muste. Sensory evaluation of bakery products and its role in determining of the consumer preferences. Journal of Agroalimentary Processes and Technologies. 2012;18(4):304-306.
- Raghuram T.C. Diabetes mellitus. Nutrition quarterly NIN, ICMR. 1988;22(1):3.

This work is licensed under a Creative Commons Attribution 4.0 International License.






