Introduction
A recent systematic review and meta-analysis1 demonstrated that vegetarians have higher levels of plasma tHcy and lower levels of serum vitamin B12 than omnivores, brought about by a lack of dietary animal products. Hyperhomocysteinemia {plasma tHcy level >15 µmolL-1as defined by2} has been shown to be linked with chronic medical conditions including cardiovascular disease (CVD).3,4 Other studies have shown that coronary heart disease (CHD) is linked to homocysteine concentrations with a substantial risk occurring at >10 µmolL-1 plasma tHcy.5,6 Furthermore, each 5 µmolL-1 increase in plasma tHcy is associated with an approximate 20% increased risk of CHD events,3,4 irrespective of diet. Using epidemiologic and clinical data, it has been suggested7 that elevated plasma tHcy is a risk factor in 82.8% of the CVD conditions examined. From these studies 71.4% of the reported CVD conditions showed that plasma tHcy levels can be employed as a biomarker for the risk of developing CVD.7
Obersby et al.,7 have suggested that normal levels of plasma tHcy need to be maintained, as a precaution to avoid increasing the risk of developing or exacerbating CVD. Methylcobalamin is the only form of vitamin B12 that contains a methyl group, and as a consequence is the only form of vitamin B12 that can directly reduce homocysteine.8
The other forms of vitamin B12 (i.e. cyanocobalamin – artificially synthesised and widely used in supplements and fortification of food and beverages, hydroxocobalamin and adenosylcobalamin) on entry to the bloodstream must be converted in the body to methylcobalamin before they can be utilised in the folate cycle for remethylation of homocysteine to methionine.9,10 This conversion process is necessary to maintain non-harmful levels of homocysteine, and in the case of cyanocobalamin may take from four to nine weeks,11 assuming that there is no disruption by genetic factors, age related issues and metabolic problems.1
In order to test the hypothesis that supplementary methylcobalamin can normalise elevated plasma tHcy of vitamin B12 deficient vegetarians, a clinical trial was therefore needed. However, it is highly unlikely that an accurate calculation of the sample size of a clinical trial could be made unless it was based on existing strong evidence.12,13 The calculation of the sample size required to reject the null hypothesis (H0) needs to be based on evidence from previous studies of the difference likely to be found between experimental and control groups. The paucity of published data in relation to this is reflected by the fact that just one published study by Yajnik et al.,14 could be located that tested the effectiveness of methylcobalamin to lower plasma tHcy in female Indian vegetarians. However, this was a proof of principle (POP) study. The duration of the study was just six weeks which may be too short to achieve the full effect of methylcobalamin supplementation. Furthermore, the dose size of 500µg taken every alternate day may not be sufficient to normalise the elevated plasma tHcy of vitamin B12 deficient lactovegetarians. This assertion is supported by the results shown within Table 2 of the study by Yajnik et al (i.e. mean baseline 18.4µmolL-1 to mean post treatment 13.4µmolL-1). These authors cited a study by Kwok et al.,15 which was specifically aimed at showing that vitamin B12 supplementation improves arterial functions in vegetarians with subnormal vitamin B12 status. This study was a placebo controlled crossover trial with vitamin B12 (500µg/day) taken over twelve weeks with ten weeks washout, followed by a further 24 weeks of vitamin B12 treatment However, the type of vitamin B12 employed and how it was administered was undisclosed. The results of that study demonstrated a reduction in plasma tHcy, but vitamin B12 did not normalise the level of plasma tHcy (i.e. mean 16.7µmolL-1 at baseline to a mean 11.3µmolL-1 following treatment). The conflicting findings from this study could be a result of the particular rout of administration of vitamin B12 or the relatively short washout period of the ten weeks.16 Both the Yajnik et al and Kwok et al studies failed to normalise homocysteine levels to < 10µmolL-1.5,6
Materials and Methods
The investigation reported in this paper is the first clinical pilot study to effectively explore the normalisation of elevated plasma tHcy of vegetarians by the direct intervention of oral methylcobalamin.
Ethical Consideration
The clinical pilot study was conducted according to the guidelines laid down in the Declaration of Helsinki17 and all procedures involving human subjects were approved by the University of West London Research Scrutiny & Ethics Sub-Committee. Written informed consent was obtained from all subjects.
Registration
The clinical pilot study was registered with ClinicalTrials.gov Protocol Registration System
08 June 2012 and allocated the registration number NCT01661309.
Participants
Over the period July 2012 to December 2013 a total of 49 volunteers living in the UK were recruited via the Vegetarian Society and the Vegan Society, and who had been practicing vegetarianism for >3 years were approved to participate in the clinical pilot study. These subjects comprised lactovegetarians (LV), lactoovovegetarians (LOV) and vegans. In our study LVs and LOVs were treated as one group, since there is no nutritional detrimental difference. Whilst LOVs consume eggs that contain traces of vitamin B12, they also contain vitamin B12 cobamides that block absorption of the actual vitamin B12 and increase the body’s need for this nutrient.18
Inclusion criteria
All participants of the study successfully completed a diet, supplements & medication, medical
history and lifestyle confidential questionnaire and fulfilled the following criteria: Have a measured plasma tHcy of ≥ 10 µmolL-1, aged between 18 and 65 years old, not participating in a weight reducing diet, not consuming regularly supplementary vitamin B12 > 10µg/day, not suffering from pernicious anaemia or other conditions resulting in vitamin B12 deficiency, not previously undergone bowel surgery or suffered from gastrointestinal disease, not pregnant, lactating or trying to conceive, a non-smoker, not consuming alcohol regularly (> 2 units/day for females, > 3units/day for males); not consuming caffeine on a regular basis (> 4 cups/day of strong tea or coffee), not suffering from genetic metabolic disease, not suffering from renal failure, diabetes, thyroid disease, CVD, dementia or cancer, not using medications known to influence nutritional status and not suffering a known blood-borne infection (e.g. Hepatitis or HIV).
From the 49 participants admitted to the study, ten either withdrew or were discounted for breaching the study protocol. In order to avoid overoptimistic estimates of the efficacy of methylcobalamin, statistical analysis was performed with the noncompliance and missing outcomes being excluded (n=39) and included (n=49) in the calculations. In the case of the inclusion of the withdrawn subjects (n = 49), intention to treat (ITT) analysis was included on the basis of using the strict rules of last observation carried forward (LOCF) technique.19
The reason why the ten ITT subjects withdrew or were discounted from the study was: From the methylcobalamin group, four became omnivores; one failed to have a post treatment homocysteine test taken. From the placebo group, one failed to supply any food diaries; one was due to poor
health; two disliked the treatment schedule; and one started taking high daily doses of vitamin B12.
The design and structure of the clinical pilot study was a double blind randomised placebo controlled trial with two arms. The participants, principal investigator and statistician were all unaware of the identity of the methylcobalamin and the placebo groups.
The subjects were randomly assigned to each arm, according to an Fx-115ms computer generated simple randomisation list. The oral methylcobalamin arm was an 1mg lozenge supplied and certified by Jarrow Formulas Inc, Los Angeles, USA. The rationale for choosing the dose size and frequency of consumption of the methylcobalamin was to ensure that there was an effect in the duration of the study, which also took into account any inadvertent dosage changes due to possible methylcobalamin instability.
The oral placebo arm was a lozenge supplied and certified by Lonsdale Health Products Limited, Ingleton, UK. Each participant conducted a baseline plasma tHcy measurement by means of an accredited and validated blood self-sample testing kit, supplied by YORKTEST Laboratories Limited, York, UK. Each group dissolved one lozenge in the mouth, following a meal, every other day for sixteen weeks. A detailed seven day diet diary for the first and final weeks of the study was provided by each participant, which was supervised by a Nutritional Therapist. A post treatment homocysteine measurement was taken by each subject using a further self-sample testing kit supplied by YORKTEST.
The lozenge type of methylcobalamin dissolved in the mouth was preferred over a swallowed whole
tablet because it has been shown that vitamin B12 not dissolved in the mouth can be up to 88% mal-absorbed (20), due to the lack of R-binder mostly obtained from saliva, which is required to start the absorption process.
Data collection and distribution of lozenges:
- Each participant was allocated an Fx-115ms computer generated randomised code number.
- Distribution of the lozenges by the study supervisor was in two containers each holding 28 lozenges of either type A or type B.
- Participants, Principal Investigator and Statistician were unaware which arm of the study the participants belong to, and to the identity of lozenges A and B.
- Compliance was checked by counting unused lozenges following the return of the containers.
The analysis of the outcome of the study took place at the University of West London, UK, from
the supervised diet diaries provided by the participants, and plasma tHcy measurements certified by YORKTEST, on an ‘ongoing’ basis.
A pictorial representation of the clinical pilot study is presented in Figure 1.
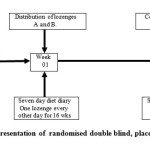 |
Figure 1: Pictorial representation of randomised double blind, placebo controlled, clinicalpilot study. Click here to View figure |
Homocysteine Assay
The YORKTEST self-sample system enables immediate separation of blood plasma, so that a finger prick blood sample can be collected using a sterilised lancet. The sample is taken on arising in the morning, following an overnight fast. The device immediately separates the blood cells and collects the plasma in a collection disc. The sample is returned by post, which would be received by YORKTEST well within the stability life of the returned sample, which is up to ten days , even when stored at 37oC.21 YORKTEST have patented this system and hold accreditation to the relevant EC Directives.
Statistical Analysis
Statistical analysis of the results was performed with IBM Corp SPSS software, version 21.
A ‘Paired Samples t Test’ was performed for changes in plasma tHcy with the null hypothesis (H0)
being defined as ‘there will be no change in plasma tHcy following treatment’. H0 was rejected if the change in plasma tHcy was significantly different from zero, but accepted if it was not significantly different from zero.
Baseline and post treatment mean, SD, P and CI95% values of plasma tHcy for the methylcobalamin and placebo groups for participants who completed the study (n=39) and which contained the ITT subjects were also tabulated.
Also, following analysis of the diet diaries of the participants who completed the pilot study (n=39) the mean and SD of daily intakes of nutrients which are involved in the bio-regulation of homocysteine levels were calculated for the first and final weeks of the study and compared with RDA and daily adequate intake (AI) values. In view of the fact that the generation of homocysteine is totally dependent on the amino acid methionine,22 the methionine content of the participants’ diet diaries was compared with the baseline plasma tHcy, to establish if a correlation exists.
Results
The socio demographic characteristics of age, gender, and vegetarian classification of the participants of the pilot study are presented in Table 1.
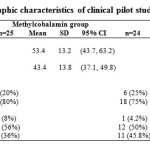 |
Table 1: Socio demographic characteristics of clinical pilot study participants Click here to View table |
The comparison of mean values and SD’s of baseline and post treatment values of plasma tHcy, for subjects who completed the pilot study and the group containing ITT subjects are presented in Table 2.
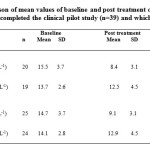 |
Table 2: Comparison of mean values of baseline and post treatment of plasma tHcy, for participants who completed the clinical pilot study (n=39) and which contained the ITT subjects (n=49) Click here to View table |
Table 2: Comparison of mean values of baseline and post treatment of plasma tHcy, for participants who completed the clinical pilot study (n=39) and which contained the ITT subjects (n=49)
There were no reported adverse events from the treatments reported by the participants who completed the study.
Comparison of the nutrients which are involved in the bio-regulation of homocysteine levels and RDA and AI values are presented in Table 4A and Table 4B.
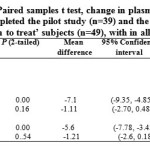 |
Table 3: Paired samples t test, change in plasma tHcy, for participants who completed the pilot study (n=39) and the group containing ‘intention to treat’ subjects (n=49), with in all cases test value = 0. |
![Table 4A Comparison of daily intake of nutrients and have intake of nutrients involved in the bio-regulation of homocysteine levels of participants who completed the clinical pilot study (n=39), taken from the diet diaries for the first seven days of the study. [RDAs and AIs taken from the Institute of Medicine of the Academy of Science (23). Dietary nutrients are in accordance with Foods Standards Agency (24) and USDA Agricultural Research Service (25)]](http://www.foodandnutritionjournal.org/wp-content/uploads/2015/12/Vol3_No3_Effi_Ober_T4A-150x150.jpg) |
Table 4 (A): Comparison of daily intake of nutrients and have intake of nutrients involved in the bio-regulation of homocysteine levels of participants who completed the clinical pilot study (n=39), taken from the diet diaries for the first seven days of the study. [RDAs and AIs taken from the Institute of Medicine of the Academy of Science.(23) Dietary nutrients are in accordance with Foods Standards Agency (24) and USDA Agricultural Research Service (25)] Click here to View table |
![Table 4B. Comparison of daily intake of nutrients and have intake of nutrients involved in the bio-regulation of homocysteine levels of participants who completed the clinical pilot study (n=39), taken from the diet diaries for the final seven days of the study. [RDAs and AIs taken from the Institute of Medicine of the Academy of Science (23). Dietary nutrients are in accordance with Foods Standards Agency (24) and USDA Agricultural Research Service (25)]](http://www.foodandnutritionjournal.org/wp-content/uploads/2015/12/Vol3_No3_Effi_Ober_T4B-150x150.jpg) |
Table 4 (B): Comparison of daily intake of nutrients and have intake of nutrients involved in the bio-regulation of homocysteine levels of participants who completed the clinical pilot study (n=39), taken from the diet diaries for the final seven days of the study. [RDAs and AIs taken from the Institute of Medicine of the Academy of Science.(23) Dietary nutrients are in accordance with Foods Standards Agency (24) and USDA Agricultural Research Service (25)] Click here to View table |
In Table 4A and Table 4B, it was deemed unnecessary to conduct a test of significance for mean nutrient levels (except vitamin B12) that are equal to or exceeded the RDA. With regard to the mean intake of TMG, a point value for the AI was taken as 750mg. All groups with the exception of male vegans (due to small sample) were found to be all significantly less than the AI, for both the first and final seven days of the diet diaries. The choline mean intake for all groups with the exception of male vegans (due to small sample) was found to be all significantly less than the AI for both the first and final seven days of the diet diaries.
The mean vitamin B12 for the first and final days of the diet diaries, female LV-LOVs are significantly higher than the RDA, whilst both genders of vegans are significantly less than the RDA. This also applies to male LV-LOVs for the first seven days of diet diaries.
Only female LV-LOVs for the first seven days of the diet diaries contain mean levels of
vitamin B12 that is significantly higher than the RDA, whilst both genders of LV-LOVs significantly meet the RDA for the final seven days of the diet diaries.
The mean vitamin B12 for the first and final days of the diet diaries, female LV-LOVs are significantly higher than the RDA, whilst both genders of vegans are significantly less than the RDA. This also applies to male LV-LOVs for the first seven days of diet diaries.
Only female LV-LOVs for the first seven days of the diet diaries contain mean levels of
vitamin B12 that is significantly higher than the RDA, whilst both genders of LV-LOVs significantly meet the RDA for the final seven days of the diet diaries.
It was observed from the confidential questionnaire, completed by all applicants that 53%
(n = 34) were oblivious to the potential detrimental effect to health of elevated plasma tHcy, as a result of a deficiency of vitamin B12 in vegetarian diets.
Analysis of the diet diaries of the participants who completed the study strongly indicate (R2 = 0.79)
that there exists a positive correlation between baseline plasma tHcy and mean dietary methionine intake of the form Y=A.ln(X)-C (see Figure 2) of vegetarian deficient vegetarians. This dispersed following methylcobalamin intervention due to the normalisation of participants’ plasma tHcy.
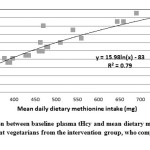 |
Figure 2: Correlation between baseline plasma tHcy and mean dietary methionine intake, for vitamin B12 deficient vegetarians from the intervention group, who completed the clinical pilot study. Click here to View figure |
Discussion
The statistical results presented in Table 2 demonstrate that methylcobalamin reduced mean baseline plasma tHcy level of 15.5µmolL-1 (n=39) to a post treatment plasma tHcy level of 8.4µmolL-1 (P<0.001).
In the ITT group this also demonstrated that methylcobalamin reduced a mean baseline plasma tHcy level of 14µmolL-1 (n=49) to a mean post treatment plasma tHcy level of 9.1µmolL-1 (P<0.001).
Both sets of results indicate that methylcobalamin normalises plasma tHcy levels, whereas, the placebo failed to achieve this.
The above results are supported by the results presented in Table 3, which demonstrates that for subjects that completed the trial (n=39) and the ITT group (n=49) H0 can be rejected for the methylcobalamin group, since P<0.05 and CI95% does not pass through zero. In both the placebo groups H0 is accepted, since P>0.05 and CI95% passes through zero.
No previously published trials were found that could be directly compared with the outcomes of the present study.
The very positive effect of methylcobalamin on lowering plasma tHcy leads to the conclusion that methylcobalamin can even at this pilot study stage be recommended as a food supplement for all categories of vegetarianism, to help maintain homocysteine at non-harmful levels.
Since methylcobalamin was administered in the lozenge form, this ensured that absorption took place by mediated intrinsic factor, non-intrinsic mediated diffusion and sublingual intake. This is particularly advantageous to individuals who cannot readily absorb vitamin B12 by mediated intrinsic factor due to autoimmune problems, resulting in partial or full pernicious anaemia.26-28
Table 4.9A and Table 4.9B illustrates that those subjects completing the study consumed at least the
RDA and AIs range of mean values of nutrients that can influence homocysteine reduction with the exception of vitamin B12 for vegans and male LV-LOVs and both genders for LV-LOV and vegans for choline and trimethylglycine (TMG). However, the TMG reaction for the remethylation of homocysteine, can only take place in the liver and kidney of human beings as the enzyme involved, betaine homocysteine methyltransferase, is not present in other organs of the body.29 The influence on elevated plasma tHcy is therefore considered to be minimal in the TMG reaction.
Vitamin B12 was not measured since there are no accredited or validated assays available that have sufficient sensitivity and specificity to measure methylcobalamin that has been absorbed into cells. Some participants independently arranged for their physician to have their vitamin B12 status measured. In most cases the results indicated that their vitamin B12 status was normal
i.e. > 150pmolL-1,30 yet their homocysteine level was found to be elevated. This is explained by the fact that NHS vitamin B12 assays measure total serum vitamin B12.31 The standard NHS vitamin B12 assay measures total plasma cyanocobalamin, following chemical modification of the other forms of cobalamin to cyanocobalamin by potassium cyanide. The procedure renders the assay impossible to identify each fraction of vitamin B12 being measured. As a consequence, it can be reasonably deduced that under these circumstances these participants were actually methylcobalamin deficient leading to a rise in plasma homocysteine levels.
Verification of participant methylcobalamin deficiency is strongly indicated by the fact that these participant plasma tHcy was normalised (i.e. < 10µmolL-1) by the intervention of methylcobalamin during their participation in the present clinical pilot study.
It is very clear from the results of the clinical pilot study and analysis of the participants’ diet diaries which show that the diets are rich in the homocysteine lowering nutrients. In addition, participants exhibited subnormal levels of methylcobalamin, resulting in elevated plasma tHcy, which according to the results of the study have been normalised, probably due to: The type of intervention employed, dose size, duration of treatment, methylcobalamin supplement dissolved in the mouth and therefore mixed with saliva.
In conclusion, the primary objective was successful since the results of this study strongly suggest that supplementary methylcobalamin will normalise elevated plasma tHcy of vitamin B12 deficient vegetarians provided that they are not deficient in other bio-regulation of homocysteine nutrients and enzymes. According to Huang et al.,32 vitamin B6 and folate have little or no effect on plasma tHcy concentration when individuals have adequate dietary vitamin B6 and folate intakes. Furthermore, it will allow an accurate sample size to be calculated for a further definitive clinical trial. Analyses indicate that the RDA for vitamin B12 maybe too low. This supports previous research,33 which demonstrates that doses of vitamin B12 of ≥ 6µg/day appear to be sufficient to maintain a steady-state concentration of serum vitamin B12.
It was discovered that a logarithmic relationship exists between baseline plasma tHcy of
vitamin B12 deficient vegetarians and dietary methionine, which no longer exists, following intervention by methylcobalamin.
Acknowledgements
We would like to thank all respondents for their participation in the clinical pilot study. Furthermore, our thanks go out to the Vegetarian and the Vegan Societies for their help in recruiting the participants of the study, without which the research project could not have taken place. Also, our thanks are extended to YORKTEST Laboratories Limited for supplying the homocysteine test kits, testing and validating the test results of the participant blood samples and Jarrow Formulas Inc USA and Lonsdale Health Products Limited UK for supplying the methylcobalamin and placebo lozenges employed in the study.
References
- Obersby D, Chappell DC, Dunnett A, Tsiami AA. Plasma total homocysteine status of vegetarians compared with omnivores: a systematic review and meta-analysis. Brit J Nutr; 109: 785-794: (2013).
CrossRef - Ravaglia G, Forti P, Maioli F, et al. Apolipoprotein Ee4 allele affects risk of hyperhomocysteinemia in the elderly. Am J Clin Nutr; 84: 473-1480: (2006).
- Ueland PM, Refsum H, Beresford M et al. The controversy over homocysteine and cardiovascular risk. Am J Clin Nut; 72: 324-332: (2000).
- Humphrey LL, Fu R, Rogers K et al. Homocysteine level and coronary heart disease: a systematic review and meta-analysis. Mayo Clin Proc: 83 (11): 1203-1212: (2008)
CrossRef - Malinow MR, Bostom A G, Krauss RM. Homocysteine, diet, and cardiovascular disease: a statement for healthcare professionals from the Nutrition Committee, Am Heart Assoc Circ; 99: 178-182: (1999).
- Ubbink JB. What is a desirable homocysteine level? Carmel R Jacobsen, D.W editors. Homocysteine in health and disease. Camup; 485-90: (2001).
- Obersby D, Chappell DC, Tsiami AA. Plasma total homocysteine and its relationship with cardiovascular disease. J Nutr Ther; 2: 182-193: (2013).
- Herrmann W, Obeid R, Schorr H, et al. The usefulness of holotranscobalamin in predicting vitamin B12 status in different clinical settings. Curr Drug Meta; 6 (1): 47-53: (2005).
CrossRef - Cooper BA and Rosenblatt DS. Inherited defects of vitamin B12 metabolism. An Rev Nut; 7: 291-320: (1987).
CrossRef - Pezacka E, Green R, Jacobsen DW. Glutathionylcobalamin as an intermediate in the formation of cobalamin coenzymes. Arc Biochem Biophysics; 2: 443-450: (1990).
CrossRef - Kelly G. The coenzyme forms of vitamin B12: towards an understanding of their therapeutic potential. Alt Med Rev; 2(6): 459-471: (1997)
- Whitley E & Ball J. Statistics review 4: sample size calculations. Crit Care; 6: 335-345: (2002).
CrossRef - Kirby A, Gebski V, Keech C. Determining the sample size in a clinical trial. Med J Aust; 256-257: (2002).
- Yajnik S, Lubree HG, Thuse NV, et al. Oral vitamin B12 supplementation reduces plasma total homocysteine concentration in women in India. Asia Pac J Clin Nutr; 103-109: (2007).
- Kwok T, Chook P, Qiao M et al. Vitamin B12 supplementation improves arterial function in vegetarians with subnormal vitamin B12 status. J Nutr Health & Ageing; 16 (6): 569-573: (2012).
CrossRef - Madry E, Lisowska A, Grebowiec P, et al. The impact of vegan diet on B12 status in healthy omnivores: five year prospective study. Acta Scie Polo Tech Alim; 11(2): 209-12: (2012).
- WMA Declaration of Helsinki. (1964) Ethical principles for medical research involving human subjects. http://wma.net/en/30 publications/10policies/b3/ (accessed 25 January 2012.
- Doscherholmen A, McMahon J, Ripley D. Inhibitory effect of eggs on vitamin B12 absorption: description of a simple ovalbumin Co-vitamin B12 absorption test. Brit J Haem; 33: 261-272: (1976).
- Gupta SK. Intention to treat concept: a review. Perspect Clin Res; 2(3): 109-112: (2011)
CrossRef - Crane MG. Vitamin B12 studies in total vegetarians. J Nutr Med; 4: 1-14: (1994).
CrossRef - Hart G. Measurement of homocysteine. Nutr Pract; 10: (2): 4-7: (2009).
- Chou JY. Molecular genetics of hepatic methionine adenosyltransferase deficiency. Pharm Thera; 85: 1-9: (2000).
CrossRef - Institute of Medicine of the National Academy of Science (2012) Essential guide to nutritional requirements. www.nal.usda.gov/fnic/DRI/Essential_Guide/DRIEssentialGuideNutReg.pdf (accessed January 2015).
- Food Standards Agency (2002) McCance and Widdowson’s The Composition of Foods, sixth summary edition. Cambridge: Royal Society of Chemistry.
- USDA Agricultural Research Service (2014) National Nutrient Database for Standard Reference Release.6; ndb.nal.usda.gov/ndb/search/list (accessed June 2014).
- Andres E, Loukili NN, Noel E, et al. Vitamin B12 (cobalamin) deficiency in elderly patients. Can Med Assoc J; 171 (3): 251-259: (2004).
CrossRef - Berlin H, Berlin R, Brante G. Oral treatment of pernicious anemia with high doses of vitamin B12 without intrinsic factor. Acta Medi Scand; 184: 274-258: (1988).
- Sharabi A, Cohen E, Sulkes J et al. Replacement therapy for vitamin B12 deficiency: comparison between the sublingual and oral route. Br J Pharmacol; 56 (6): 635-638: (2003).
CrossRef - Finkelstein JD, Kyle WE, Harris B. Methionine metabolism in mammals: regulatory effects of s-adenosylhomocysteine. Arch Biochem; 165: 770-779: (1994).
- National Academy of Sciences: Institute of Medicine, Food and Nutritional Board. (1998) Dietary reference intakes for thiamine, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin and choline. http://ods.nih.gov/Information/DietaryReference intakes.aspx (accessed 24th February 2014).
- NHS Direct. (2014) Anaemia, vitamin B12 and folate deficiency. www.nhsdirect.wales.nhs.uk (accessed November 2014).
- Huang YC, Chang SJ, Chiu CT, et al. The status of plasma homocysteine related to B-vitamins in healthy young vegetarians and non-vegetarians. Euro J Nutri; 42(2): 84-90: (2003).
CrossRef - Bor MV, Lydeking-Olsen E, Meller J et al. A daily intake of approximately 6µg vitamin B12 appears to saturate all vitamin B12 related variables in Danish postmenopausal women. Am J Clin Nutri; 83: 52-58: (2006).

This work is licensed under a Creative Commons Attribution 4.0 International License.






