Introduction
Industrialization and urban growth are occurring at an unprecedented rate, in this previously predominant agrarian society which promoted people to migrate from rural to urban areas and forcing them to have their meals at any place at an inexpensive rate. Both developed and developing countries are facing the problem of water and food borne diseases. One third of the population is estimated to be affected by food borne diseases each year in the developing countries.1
Seventy six million food borne illnesses has been estimated to occur annually in the United States, which resulted in 325,000 hospitalizations and 5000 deaths every year. Annually, the estimated cost of the most common food borne illnesses in the United States is around $6.5–$34.9 billion.2 According to the available reports, 1.8 million people have died from diarrhoeal diseases in 2005 globally.3
According to Center for Disease Control and Prevention (CDCP) report, each year an average of 1329 food borne disease outbreaks have been reported between 1998 and 2002. Among which 52% of the incidents were observed in food service establishments.4 During the same period, the Oregon Public Health Division reported 5% of food borne diseases.5 Similarly, Zain and Naing,6 have reported 10-20% of food-borne disease outbreaks in Malaysia are due to contamination by the food handlers.
Food handlers is any person who handles food, regardless whether he actually prepares or serves it, play a vital role in the prevention of contamination associated with the spoilage of food and food poisoning during the preparation, production, processing and distribution of food.7 If their personal hygiene is not satisfactory, it may lead to the contamination of the raw food and processed food stuffs. Similarly, asymptomatic carriers of pathogenic organisms in food handling may lead to transmission of food borne diseases among the consumers.2,8
In the recent past, due to changing lifestyle, breakdown of joint family system and increase in number of working women has led to consumption of ready to eat foods. Nowadays majority of the individuals are able to satisfy their taste and nutrition needs, but they pay little attention to health, hygiene and food safety.9 The present study aimed to evaluate the health status of food handlers of eating establishments in and around Coimbatore district, South India.
Materials and Methods
Study Design
This is a cross sectional study conducted in food establishments (hotels and messes) in and around Coimbatore, South India. Food handlers with no clear decision on a given question were asked not to mark any options for that question. Each questionnaire took approximately 20 minutes to complete. Data was collected only during the weekends.
Study Sample
The study was carried out between July 2012–June 2013, amongst food handlers working in 19 food establishments (12 hotels and 7 messes) located in the study area. Of the 245 food handlers working in these food establishments, 163 food handlers (66.5%) participated in the study. Those food handlers 82 (33.5%) could not be contacted during the visit were excluded from the study.
Study Method
A self-administrable questionnaire was developed for this study with 29 multiple choice questions with four, five or six possible answers, including ‘‘do not know” and ‘‘other”, for the purpose of minimizing the possibility of selecting the correct answer by chance. This study was conducted with the aim of exploring the socio demographic characteristics of respondents such as age, gender, educational level, duration of experience, type of settlement, type of food establishment and income. The information regarding their health status, illness in previous months, addiction such as smoking, alcohol and betel chewing were also collected.
Data collection and analysis
Information from food handlers was collected using interview schedule and data thus collected are compiled and analyzed.
Results
In this study, out of 245 food handlers enlisted, 163 food handlers were examined in the 19 food establishments (12 hotels and 7 messes) are given in Table 1. Table 2 reveals that the vast majority of food handlers 80.37%131 were males. The maximum number of food handlers were cooks 26.91% and cleaners 20.25%.33 Similarly, the majority of food handlers 61.96%101 were from rural area, compared with urban and slum. Unmarried workers are 53.99%88 and whereas married workers were found to be 46.01%.75 Among 163 food handlers, 49.69%81 were having 1 to 5 years of experience, 32.52%53 were having more than 5 years of experience and 17.79%29 food handlers were having less than 1 year of experience.
 |
Table 1: Hotels and Messes Surveyed During Study |
 |
Table 2: Distribution of Food Handlers According to their Socio-Demographic Profile Click here to View table |
The income of the food handlers is classified into 4 categories in Table 2, out of 163 food handlers 19.04%32 belongs to less than Rs.2000 categories, 20.24%33 belongs to Rs 2001-3000 category, 24.53%40 belong to Rs 3001-4000 category and 35.58%58 belong to above Rs. 4001 category. As shown in Table 3, the majority of food handlers 26.38%43 were between the age group of 15-24 and 35-44 years, 26.99% 44 were between 25-34 years, 17.79%29 were between 45-54 years, 2.45% were above 55 years of age respectively.
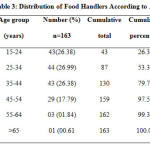 |
Table3: Distribution of Food Handlers According to Age Click here to View table |
Table 4 depicts that out of 163 food handlers 22.69%37 were illiterate, 22.09%36 studied primary, 23.93%39 studied middle school, 19.63%32 studied secondary school and 11.66%19 studied above secondary school. Table 5 shows the morbid condition of the food handlers, among which 62.74%32 of them were apparently healthy, 23.52%12 food handlers are prone to injuries, 19.60%10 to fever and hypertension, 10%5 to anemia, diabetes and poor nutritional status.
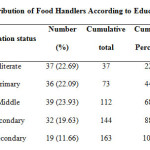 |
Table 4: Distribution of Food Handlers According to Educational Status |
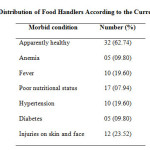 |
Table 5: Distribution of Food Handlers According to the Current Morbidity Click here to View table |
Table 6 reveals that 30.06%49 were smokers, 14.72%24 were alcoholics and 8.58%14 were addicted to both smoking and alcohol, 13.49%22 were addicted to betel chewing. Interestingly 54.60%89 were found to be free from any other common addictions. From Table 7 it was observed that 68.09%111 food handlers suffered from various diseases and 31.90%52 were not prone to any diseases. Morbidity suffered has been depicted in table 8 in order of enormity.
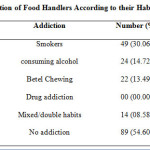 |
Table 6: Distribution of Food Handlers According to their Habits and Addiction Click here to View table |
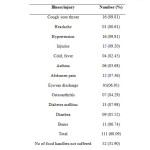 |
Table 8: Illness/Injuries Suffered by the Study Population in Previous Months Click here to View table |
Discussion
Despite the practice of technological advancement in ensuring the quality and safety of food is available, still outbreaks of food borne disease are continuing to be reported. The factors that are mostly identified for the food borne diseases are contaminated raw foods/ingredients, and poor personal hygiene of food handlers (Report of the FDA retail food programs)10. In their study, Udgiri and Masali,11 reported that 73.2% of food handlers were under 30 years of age and only 2.72% were above 50 years, even in the present study 79.75%.130 of the food handlers were under 44 years and only 2.45%4 were above 55 years. In a similar, Gupta and Ketkar12 from Nagpur reported 22.03% of the food handlers were under 25 years of age. In this study, the majority of food handlers were from rural area (61.96%,101 while 31.90%52 were belong to urban and 6.13%10 were from the slums.
In a similar study by Zain and Naing6 and Isara and Isah,7 69.50%, and 65.10% were females respectively, but we have observed 80.37% 131 of food handlers were males. In the current study, 22.69%37 of food handlers were found to be illiterate and 77.30%126 of food handlers were found to have completed their formal education, which differed markedly,7 where they reported that 98% of respondents had completed the formal education. These findings differ from our study, in which 30.06%49 were smokers, 14.72%24 were alcoholics and 8.58%14 were addicted to both smoking and alcohol, 13.49%22 were addicted to betel chewing and about 54.60%89 were free from any other common addictions.
Food handlers were found to suffer from majority of morbid condition like diabetes, hyper tension, injuries, anemia, asthma, cough, fever, and abdomen pain. Amongst all these, hyper tension, diabetes, injuries, burns, cough and anemia were found to be common. In the present study, 68.09%111 of food handlers reported some illness in the previous 3 months. The food handlers morbid status are depicted in Table 5 in order of magnitude, history of illness was restricted to 3 months for the purpose of better recall. Rathore13 observed that (25.33%) of food handlers suffered from one or more disease in the past 6 months. Anemia were found in (9.80%) of food handlers. Chitnis14 who had observed 74.13% of overall morbidity, and also found that anemia (22.13%) was most frequently seen morbid conditions.
Conclusion
The results obtained from the present study could be the baseline data to improve the health status and create an educational awareness program to improve the food safety practices and behaviour of food handlers. By adapting good hygienic practices by food handlers would promote the trust between consumers and food establishments. Moreover, the supervisor should confirm that the food handlers wear hand gloves, hair net either during preparation, serving and packing etc. Therefore this study suggests, frequent medical checkup (at least once in 6 months), training in personal hygiene and organizing food safety practices by the owners will considerably increase the knowledge of the food handlers in food handling to prevent the food borne diseases.
Acknowledgments
Authors are grateful to the Management of Karunya University, Coimbatore, India for their kind support to carry out this publication.
References
- Schlundt, J., Toyofuku, H., Jansen, J. & Herbst, S. A. Emerging food-borne zoonoses. Sci. Technol. Rev., 23, 513-515 (2004).
CrossRef - Mead, P. S., Slutsker, L., Dietz, V., Mccaig, L. F., Griffin, C. & Shapiro, J. S. Food related illness and death in the United States. Emerg. Infect. Dis., 62, 607-625 (1999).
CrossRef - WHO, 2007. Prevention and control of intestinal parasitic infections. Geneva: World Health Organization. 1987, pp. 7-18.
- Jones, T. F. & Angulo, F. J. Eating in restaurants: A risk factor for food borne disease?. Clin. Infect. Dis., 43, 1324-1328 (2006).
CrossRef - DeBess, E. E., Pippert, E., Frederick, J. A. & Paul, R. C. Food handler assessment in Oregon. Foodborne Pathog. Dis., 6, 329-335 (2009).
CrossRef - Zain, M. M. & Naing, N. N. Socio-demographic characteristics of food handlers and their knowledge, attitude and practice towards food sanitation: A Preliminary report. Southeast Asian J. Trop. Med. Public Health., 33, 410-417 (2002).
- Isara, A. R. & Isah, E. C. Knowledge and practice of food hygiene and safety among food handlers in fast food restaurants in Benin City, Edo state. Niger. Postgrad. Med. J., 16, 207-212 (2009).
- Pitchard, C., Walker, E. & Forsythe, S. Food handlers’ hygiene knowledge in small food businesses. Food Control., 14, 339-343 (2003).
CrossRef - Santosh, M. J., Nogueira, J. R. & Patarata, L. Knowledge levels of food handlers in Portuguese School canteens and their self-reported behaviours towards food safety. Int. J. Environ. Health. Res., 18, 387-401 (2008).
CrossRef - Udgiri, R. S. & Masali, K. A. A study on the health status of food handlers employed in food establishments in Bijapur city. Ind. J. Comm. Med., 32, 131-132 (2007).
CrossRef - Gupta, S. C. & Ketkar, Y. A. Prevalence of Intestinal Parasites in food handlers. Ind. Med. Gazzete., 15, 295-298 (1981).
- Rathore, A. S. An evaluation of health status of food handlers and sanitary status of messes, of training establishments in Karnataka. Ind. J. Comm. Med., 18, 21-25 (1983).
- FDA, 2000. Report of the FDA retail food program database of food borne illness risk factors. Center of Food Safety and Applied Nutrition, 2000.
- Chitnis, U. K. B. An evaluation of health status of workers in eating establishments in Pune Cantonment. Med. J. Armed. Forces., 2, 34-35 (1986).

This work is licensed under a Creative Commons Attribution 4.0 International License.






