Introduction
World Health Organization (2000) has labeled obesity as a “global epidemic” and estimated that billion people worldwide are overweight and 300 million are obese.1 The prevalence of obesity has been increasing globally and its impact on public health is marked in both developed and developing countries. Globally, an estimated 10 percent children, between 5 to 17 years of age, are overweight or obese. Many developing countries especially those undergoing rapid nutrition transition like India are also witnessing the emergence of this problem.2
Adolescence has been proposed as critical period for the development of obesity.3 Therefore interventions initiated during adolescence lay a strong foundation for lifetime health related behavior and inculcate healthy behavior leading to long-term benefits rather than short term benefits. Physical activity is an ideal focus for intervention because it has many other benefits in addition to adiposity regulation.4 Similarly, physical activity interventions are more feasible for implementation because children are fond of outdoor play and increasing physical activity in form of attractive games is easier to implement than dietary intervention that often involves restriction of foods that are favorite to children.
Most of the intervention studies for management of obesity are from the Western countries where school based approach are used as more than 95 % of adolescents are enrolled in school making it an ideal setting to reach large number of children and adolescents. Almost all studies revel that action taken to reduce adolescent obesity through increased physical activity appears to be an encouraging area.5-8 However, despite of these positive results for the treatment of adolescent obesity there are very few intervention studies in India for management of adolescent obesity.
Materials and Methods
School going boys (n=229) from 5th to 10th standard covering the age 9-15 years were included in the study. All subjects were assessed for various anthropometric measurements like weight, height, sitting height, body fat, waist circumferences and skin folds at four sites i.e. triceps, biceps, sub-scapular and supra iliac were measured in duplicate. Along with this habitual dietary intake, habitual activity pattern and blood pressure were also measured. Body weight and height was measured using standard procedure, body fat percent was measured using Omron body fat monitor (Japan, 300) which works on bio-impedance analysis principle. Waist circumference, which provides an estimate of central adiposity was measured using a non-stretchable measuring tape with an accuracy of 0.1 cm. Skin fold thicknesses were measured on the left side of the body in duplicate to the nearest of 0.2 mm with a Harpenden’s skin fold caliper. A pediatrician measured the blood pressure using sphygmomanometer (mercury). Dietary pattern and physical activity was administered on a sub sample of subjects identified as overweight based on BMI (IOTF cut-offs) indicator and their respective age-sex matched controls selected from the remaining sample of students.
The Study was Approved by Institutional Research Advisory Committee(Pune)
The after school physical activity intervention consisted of five 60-minutes sessions per week and each session was divided in to warm-up period and stretching activities, Cardio respiratory endurance and strength activities and cooling down. Intervention consisted of a non-competitive, recreational physical activity program held after school hours in the school premises. The program consisted of 60-minutes sessions, five days/ per week for 10 months. The sessions included sports with alternative games requiring physical activity of moderate intensity. Considering holiday, weekends and examinations, a total of 148 such sessions were conducted during the academic year. After one academic year the same team collected data on anthropometric measures, diet and physical activity using the same survey tools. This data was compared with the baseline data and was used to evaluate the independent effect of physical activity intervention on adiposity at the end of academic year. Analysis was carried out using fox-pro and Statistical Package for Social Sciences (SPSS/PC Version 11.0 for Windows, SPSS Inc. Chicago IL).
Results and Discussion
The flow chart of the subjects participating in the study is given in Fig 1. At baseline 229 boys provided baseline anthropometric data. However anthropometric measurements were obtained on 205 (88.0 %) of these children at the follow-up, therefore for further analysis 205 boys were considered. Based on the recommendations for physical activity interventions among adolescents we divided subjects into three groups. The recommendations suggest 30 minutes of moderate intensity exercise for at least three days a week 9 which accounts to 450 minutes of physical activity per month (15 days x 30 min/day).
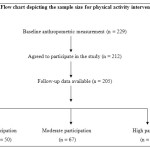 |
Figure 1: Flow chart depicting the sample size for physical activity intervention Click here to View figure |
In the current study, each activity session consisted of 50 minutes of moderated activity, therefore subjects who attended at-least 9 sessions per month (i.e. total 90 sessions over a period of ten months) met these recommendations of physical activity. Therefore, subjects who attended less than 90 sessions were defined as low participation group. Similarly, we defined a cut-off for high participation based on the report “Physical Activity and Health: A report from the Surgeon General. US Dept of Health and Human Services: Atlanta, 1996. It reports that `All people over the age of 2 years should accumulate at least 20 minutes of endurance-type physical activity, of at least moderate intensity, on preferably all days of the week’. This implies 600 min/month (20 minutes x 30 days = 600min/month). In view of the fact that the school sessions were 50 min/day, 120 sessions in ten months could correspond to high participation. Therefore, those who attended more than 120 sessions of the total 148 sessions were considered as high participation group. Those subjects who attended more than 90 sessions but less than 120 constituted the moderate participation group. Out of the total 205 boys studied, 24 % had low participation, 33 % had moderate participation and 43 % had high participation.
The intervention was aimed to increase physical activity and to examine its effect on adiposity indicators among adolescents. Therefore, data was analyzed to see the effect on adiposity indicators, changes in central adiposity indicators and changes in physical activity patterns and blood pressure levels. Each of these is discussed in the following sections.
1. Change in adiposity indicators: The anthropometric data for baseline as well as follow-up is summarized in Table 1.
 |
Table 1: Mean (± SD) anthropometric measurements at baseline and follow-up by levels of participation in physical activity intervention Click here to View table |
It can be seen that the subjects in the three groups had similar age and anthropometric measurements except body fat at baseline. At follow-up increase in weight was less (2.0 kg) among the high participation group compared to those in lower participation group (4.1 kg), but the increase in height was comparable in both the groups. Although the change in BMI was not significant children with high participation had a significant reduction in body fat (1.0 %) at follow-up. Martines et al. (2008) reported similar results where he assessed the impact of a physical activity program on obesity in primary school children.10 Martines (2008) intervention included recreational, non-competitive physical activity program conducted after school hours on school premises. The program consisted of three 90-minutes sessions per week, for 24 weeks. At the end of the intervention there were no differences in BMI between the intervention and control groups.
When skin fold measures were studied, the children from high participation group had significant reduction in triceps skin-fold and (1.3 mm) and biceps (1.2mm) skin-folds at follow-up. Edson et al. (2009) reported similar reduction in triceps skin fold thickness when he examined the influence of programmed physical activity intervention among adolescents of age range 10 to 15 years 11. We further examined the changes in prevalence of overweight at baseline and at follow-up. The changes in prevalence of overweight between baseline and follow-up using three different indicators are shown in Table 2. IOTF cut-offs12, Body fat > = 25% for boys and > =30 % for girls13, Age-sex specific 85th percentile value given by Must et al. (1991)14. ** p for trend <0.01(using Z test for proportion), ns: not significant.
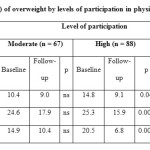 |
Table 2: Prevalence (%) of overweight by levels of participation in physical activity intervention Click here to View table |
It can be observed that the decrease in prevalence of overweight was highest among those with higher participation in the physical activity intervention using all three indicators of adiposity. Furthermore, this intervention was associated with a modest decrease in the overall prevalence of overweight using BMI or triceps as indicators. These results confirm that the physical activity intervention in the current study helped in reducing adiposity among adolescents.
2. Changes in Central adiposity indicators: High levels of central body fat are known to be more closely related to cardiovascular risk factors than with total body fat. Results of our study reveal that central adiposity is closely associated with increased risk of high blood pressure. However, there are relatively few studies that have assessed the role of physical activity as an intervention on central adiposity indicators among adolescents. We studied the effect of physical activity intervention on various central adiposity indicators like waist circumference, sub-scapular skin folds and supra-iliac skin folds. It can be observed that there were no significant differences in the mean values of these indicators of central adiposity at baseline (Table 3)
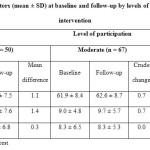 |
Table 3: Central adiposity indicators (mean ± SD) at baseline and follow-up by levels of participation in physical activity intervention Click here to View table |
At follow-up low participation group had significant gain in all the three central adiposity indicators i.e. waist circumference (1.1 cm), sub-scapular (1.4mm) and supra-iliac (0.3) skin fold. On the other hand, there was significant decrease in these three parameters among the high participation group (1.8, 1.7 and 0.7 respectively). This indicates that participation in physical activity intervention not only helps in reducing overall adiposity but also useful in reducing central adiposity among adolescents. Gutin and Owens (1999) studied the influence of 4 months of physical training (PT) on body composition among 81 obese adolescents aged 7 to 11 years wherein subjects were offered physical training program for 5 days a week for 40 min/session.15 The physical training had a favorable influence on percent fat and abdominal adipose (measured by DEXA) without dietary intervention. In the current study, subjects with high participation in physical activity intervention showed significant reduction in central adiposity as indicated through reduced waist circumference, sub-scapular skin folds and supra-iliac skin folds. Thus, these results also suggest that waist circumference and sub-scapular skin folds are sensitive indicators for assessment of changes in central adiposity among adolescents.
3. Change in physical activity patterns: Most of the interventions to date have focused on increasingphysical activity during the school day.16-18 Few researchers report that it is possible thatstudents who increase their physical activity levels duringthe school day will compensate by decreasing out-of-school physicalactivity. Therefore we studied time spent in various activities and inactivity among these subjects outside the school hours. Time spent in outdoor games which included games like cricket, basketball, badminton, football etc, did not show significant change (Table 4).
 |
Table 4: Median (range) time (minutes/day) spent in various activities at baseline and follow-up according to levels of participation in physical activity intervention Click here to View table |
Similarly, time spent in special activities including swimming, dance, karate and judo did not show significant change. This confirms that the physical activity program initiated in the study did not compensate for out of school activities. However, when inactive time and TV viewing was considered, there was a significant decrease in the time spent in inactive behavior and TV viewing among subjects with high participation in physical activity intervention. Thus this physical activity intervention also helped in decreasing time spent in inactive behavior viz. TV viewing. This was an important result of intervention as TV viewing is known to be the most important component of inactivity among adolescents. TV viewing has a negative effect on both sides of the energybalance equation i.e. it displaces active play and physical activitytime. At the same time TV viewing is known to be associated with increased food and energy intake,as an accompaniment to TV viewing and as a result offood advertising.
Thus to conclude, results from the current study show that physical activity intervention was effective in reducing adiposity and prevalence of overweight among adolescents. The reduction in adiposity was significant only among those who had high participation i.e. more that 120 sessions over a period of 10 months. This corresponds to 12 sessions of 50 minutes each per month and this can be further projected to 3 sessions per week. Thus, physical activity intervention consisting of a 50 minutes session of moderate intensity at-least thrice a week should be recommended among adolescents. In other words, school-age children should participate in 50 minutes or more of moderate physical activity at least three times a week.
4. Change in dietary intake: Further, we compared the dietary intake among these three groups to confirm that the changes in adiposity levels were are not due to difference in dietary patterns. Therefore we compared the FFQ data at baseline and at follow-up by levels of participation (Table 5). There was no significant difference at baseline among the three groups. Among the high participation group where the prevalence of overweight significantly reduced at follow-up, none of the food groups showed significant change from baseline. The data thus confirms that the reduction in the prevalence of overweight and adiposity indicators among the high participation group can be attributed solely to the effect of physical activity intervention.
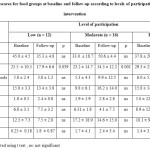 |
Table 5: Mean (± SD) scores for food groups at baseline and follow-up according to levels of participation in physical activity intervention Click here to View table |
5. Change in blood pressure levels: We studied the effect of physical activity intervention on blood pressure levels among adolescents. For this purpose, we compared mean of SBP and DBP at baseline and at follow-up according to levels of participation in physical activity intervention (Table 6).
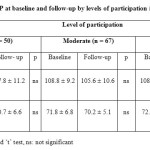 |
Table 6: Mean (± SD) SBP/DBP at baseline and follow-up by levels of participation in physical activity intervention Click here to View table |
It can be observed that mean SBP and DBP reduced among the high participation group, but did not reach statistical significance. This could be probably due to smaller sample size. Other reason could be that a longer period would be required to see the effect of intervention on blood pressure levels.
Thus to summarize our data shows that after-school program of recreational physical activity is a excellent avenue for reducing adiposity among school children. This is true as this intervention affected both physical activity and sedentary behavior which are known to be two distinct modes of behavior that independently influence adiposity. Our finding shows that school programs can promote physical activity among youths. Further, the sustainability of physical activity programs is potentially high as it is a simple and inexpensive intervention. Moreover, it achieved objective health benefits without requiring parent’s time or active participation. The results thus bring out the potential use of school as a suitable setting for the promotion of healthy lifestyles in children.
Acknowledgements
The authors are grateful to The Director, Agharkar Research Institute, for encouraging and providing the funds and facilities to carry out this work in the institute. We greatly appreciate the help of other staff members in the Department during data collection.
Conflict of Interest
There is no conflict of interest.
References
- World Health Organization (2000) World health organization (2000) Obesity Preventing and managing the global epidemic: report of a WHO consultation. Geneva: (ISBN 92-4-120894-5).
- World health organization (2004) Report on: Global strategy on diet, physical activity and health.
- Selvan M. S. and Kurpad A.V., Indian Journal of Medical Research., 120, 511 (2004).
- Goran M.I., Reynolds K.D. and Lindquist C.H., International Journal of Obesity and Related Metabolic Disorder., 23, 18 (1999).
CrossRef - Golan M, Weizman A, Apter A and Fainaru M., American Journal of Clinical Nutrition., 67 (6): 1130 – 1135 (1998)
CrossRef - Beech B.M., Klesges R.C., Kumanyika S.K., Murray D.M., Klesges L., McClanahan B., Slawson D., Nunnally C., Rochon J., McLain-Allen B., and Pree-Cary J., Ethnicity and disease. 13, s40 (2003).
- Nicklas T.A., Baranowski T., Cullen K.W. and Berenson G., Journal of American College of Nutrition, 20, 599 (2001).
CrossRef - Flodmark C.E., Ohlssan T., RydAcn O. and Sveger T., Pediatrics, 91, 880 (1993).
- Sallis J.F. and Patrick K. Physical activity guidelines for adolescents: consensus statement. Pediatric Exercise Science, 6, 302–314. Department of Health and Human Services. Physical Activity and Health: A report of the Surgeon General. Atlanta, Georgia: USDHSS, Centers for Disease Control and Prevention, 1996.
- Martinez V.V., Salcedo A.F., Franquelo G. R., Solera M. M., Sa¡nchez L. M., Serrano M. S., Lapez G. E., and Rodraguez A. F., International Journal of Obesity (Lond), 32, 12 (2008).
CrossRef - Edson S.F., Flaviano P., Wellington R.G., Carvalho E.M., Gonçalves A.D., Baldin and Gil Guerra, Journal of Pediatric (Rio J), 85, 28 (2009).
- Cole T.J., Bellizzi M.C., Flegal K.M. and Dietz W.H., British Medical Journal. 320 (7244): 1240 – 1243 (2000)
CrossRef - Williams D.P., Going S.B., Lohman T.G., Harsha D.W., Srinivasan S.R., Webber L.S., Berenson G.S., American Journal of Public Health, 82, 358 (1992).
CrossRef - Must A, Gerard E, and Dietz W., American Journal of Clinical Nutrition, 53, 839 (1991).
CrossRef - Gutin B. and Owens S., American Journal of Human Biology. 11 (2): 237 – 247 (1999)
CrossRef - Sasaki J., Shindo M., Tanaka H., Ando M., Arakawa K., International Journal of Obesity, 11, 339 (1987).
- Gutin B., Litaker M., Islam S., Manos T., Smith C. and Treiber F., American Journal of Clinical Nutrition, 63, 287 (1996).
CrossRef - Flores R., Dance for health., Public Health Reports, 110, 189 (1995).

This work is licensed under a Creative Commons Attribution 4.0 International License.






