
Introduction
The World Health Organization (WHO) defines a chronic illness as one that lasts a long period, advances slowly, and does not spread to others1. In Malaysia, non-communicable diseases (NCDs) show high mortality prevalence as the leading cause of death. NCDs are the main contributor to the global disease burden and are becoming a significant health concern in Malaysia2. According to the WHO and MOH Malaysia, 2020, NCDs and their complications pose a significant burden to Malaysia. An estimation of 3.6 million (15.6%) adult Malaysians with diabetes, 6.7 million (29.2%) with hypertension, 7.6 million (33.3%) with hypercholesterolemia, and 3.3 million (54.5%) with obesity3. Therefore, over half a million (2.5%) of adults in Malaysia are diagnosed with four NCDs. Thus, self-management is the aim to reach a consensus on the food’s influence and activities toward the prevention of NCDs at all stages of life4. In this instance, nutrition interventions are critical to reducing the risk of NCDs. Therefore, NCD prevention and control must be given top priority in public health programs. It is important to emphasise the main strategies for promoting healthy lifestyles, carrying out effective screening programs, and ensure easily available, high-quality healthcare services2.
One of the biggest challenges facing healthcare systems around the world is addressing NCDs. This is because these systems were primarily designed to provide acute episodic care rather than long-term illness management. The strategies to combat NCDs require continuity, coordination, and a comprehensive long period of supervision, observation, and care1. The significance of shifting healthcare and health policy towards chronic care systems, including primary care, was supported by substantial evidence1. The WHO recognizes the potential of telehealth to address the challenges of NCD management and improve healthcare access, particularly in underserved areas5. Telehealth ensures continuous care for patients with NCDs that would enable healthcare providers to monitor patients’ progress, nutrition, and disease management, as well as provide ongoing support.
Telehealth-enabled care coordination allows comprehensive remote patient management by integrating telenutrition services with other virtual healthcare, such as telemedicine visits and remote chronic disease monitoring6. Studies found that telehealth can be an effective tool for managing chronic diseases in primary care settings and telemonitoring technologies advance chronic disease management while reducing the healthcare system costs6-8. On the other hand, telenutrition refers to using telehealth and telemedicine technologies to provide nutrition care and counselling to patients remotely. Virtual nutrition counselling allows registered dietitians and nutritionists to provide nutritional counselling to patients in different locations. Remote patient monitoring allows providers to help monitor patients’ nutrition status, psychological condition, biomedical data, and response to interventions over time. Thus, the main aim of this review is to gather information on telenutrition intervention feasibility and effectiveness.
Materials and Methods
This systematic review follows the current guidelines for Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA)9. The detailed protocol of this study including the search strategy as well as the inclusion and exclusion criteria for study selection has been previously published elsewhere10. This review was registered on the International Prospective Register of Systematic Reviews Protocol (PROSPERO) (CRD42022340706).
Search Strategy and Study Selection
To assess the clinical feasibility and effectiveness of telenutrition for managing NCDs, this review used a combination of keywords and MeSH phrases associated with telehealth and nutrition management e.g., “telehealth”, “telenutrition”, “telecounselling”, “telediet”, “online dietetic care”, “online nutrition”, and “remote monitoring” together with “nutrition management”, “nutrition care”, “medical nutrition therapy”, and “clinical nutrition”. The databases included Scopus, PubMed, Cochrane Library, Google Scholar, and EBSCo.
The PICO framework guided the search strategy. The review focused on individuals who received telenutrition services from dietitians utilizing electronic and telecommunication technologies (apart from pregnant and pediatric populations). It evaluated the feasibility outcomes included recruitment, retention, adherence, and satisfaction, while effectiveness outcomes assessed biochemical (blood pressure, glycosylated haemoglobin (HbA1c), total cholesterol (TC), and triglyceride (TG)) and anthropometric (weight changes, waist circumferences (WC) and body mass index (BMI)) data of telenutrition in comparison to traditional in-person care. Included were comparative studies and randomized controlled trials (RCTs) published until year 2022, and available in English.
Data from systematic searches were imported into Mendeley, duplicates removed and organized in Excel. Two researchers screened titles and abstracts, while three conducted full-text screening using a Literature Review Matrix to ensure inclusion criteria were met, documenting reasons for exclusions. PDF copies of articles were stored in Google Drive, and disagreements were resolved through discussion. Data extraction recorded study details (e.g., authors, design, population, outcomes) in a Literature Review Matrix.
Risk of Bias Assessment
The quality of reporting was appraised using the Cochrane Risk of Bias tool11 and RevMan 5.0 software12. Articles were evaluated for relevancy, reliability, validity, and applicability based on randomization, intervention deviations, missing data, outcome measurement, and bias. Risks were categorized as “low,” “high,” or “some concerns.” Three researchers independently assessed quality, and funnel plots in RevMan 5.0 evaluated publication bias.
Quality of Evidence Assessment
The Modified Jadad scoring was used to determine the quality of each included study with scores of 0–4 considered as “poor,” 5–8 as “fair,” and 9–12 as “good.” The scale is based on three criteria: randomisation, double-blinding, and a description of withdrawals and dropouts13. In addition, the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system was used to assess the strength of the evidence in evaluating the outcomes, information on the number and type of studies, and assessments of the quality of evidence based on factors such as the risk of bias, inconsistency, and imprecision. It includes a summary of the overall quality of evidence and the significance of each outcome. This comprehensive approach ensures transparency and reproducibility in the evaluation of the evidence14. Then, the researchers interpreted the overall quality of the evidence for each outcome using a four-point ranked scale: 4 = high; 3 = moderate; 2 = low; and 1 = very low.
Data Analysis
All pertinent data extracted from the included studies were entered into the Literature Review Matrix, and it was then systematically summarised. Both quantitative and qualitative research articles were included in this review. To determine the feasibility and effectiveness of telenutrition intervention, a thematic analysis was used to qualitatively synthesise the results of the selected studies. To determine the feasibility and effectiveness of telenutrition intervention, a qualitative synthesis of the selected study’s findings was undertaken using thematic analysis. 15. This review extracted data based on the study’s first author and year, country, characteristics of the population (i.e. age, physical and medical condition, and nutrition management), type of intervention between intervention and control group, follow-up frequency, outcomes (feasibility and effectiveness), and results/findings. This study included data on demographic parameters, biochemical measures, baseline and final anthropometric measurements between the intervention and control groups, as well as intervention results. Additionally, the studies were pooled using statistical meta-analysis, and narrative comparisons were added as a supplement. The study characteristics—effect direction, effect size, effect homogeneity across studies, and evidence strength—were used to summarise the results. This study includes the most recent evidence on the feasibility and effectiveness of telenutrition services to undertake remote nutritional interventions employ by nutritionists and dietitians.
Using the RevMan 5.0 software, a meta-analysis was carried out, and heterogeneity was evaluated using the fixed effects model and I2 statistic12. For continuous outcomes, the mean, or standardised mean difference, was employed, whereas the risk ratio (RR) was utilised for dichotomous outcomes. An intervention was considered effective if the between-group difference was statistically significant (p-value < 0.05). For the usually homogeneous investigations, a fixed-effect model was employed. 95% confidence intervals were used to express all effect estimates16. The effectiveness of the telenutrition intervention was assessed by comparing it with traditional care in terms of biochemical measurements and anthropometric measurements.
Using funnel plots, the publication bias of systematic discrepancies between reported and unreported findings was evaluated. The funnel plot symmetry, which indicates any publication bias, was established by the p-values linked to each included study17. Furthermore, for available subgroups, more thorough comparisons between certain subgroups and subsets with comparable attributes were carried out. Each randomised controlled trial (RCT) study population’s baseline participant characteristics, including biochemical data, anthropometric measures, and recruitment strategies, may have an impact on the findings. Additionally, each study’s follow-ups may employ a varied timeframe, such as two weeks, three months, six months, or twelve months. Thus, sample sizes, study quality (i.e., follow-up schedules), and participant recruitment context, were taken into account for the results.
Results
Study Selection and Study Quality
The PRISMA flow diagram guided the article selection process, which started with identification, screening, and inclusion. The literature search for relevant articles in the Cochrane Library, PubMed, Google Scholar, EBSCo, and Scopus databases, along with citation searching, resulted in the discovery and retrieval of 3,622 articles, respectively. The database search outcomes were imported into Mendeley. The title and abstract screening process was performed for the remaining 3,450 articles after eliminating 174 duplicate articles.
In the following stage, articles were screened for records, requested for retrieval, and 51 were evaluated for full-text review eligibility. The results were then tabulated in the Literature Review Matrix for discussion. Four articles without results failed to be retrieved due to no response from the authors. The articles were sorted into two final groups (final selection and final rejection). The reasons for exclusion were recorded, which included study protocols, non-RCT studies, interventions not conducted by dietitians or nutritionists, no intervention versus control groups comparison, and paediatric study population. After a rigorous methodology of study selection, 21 articles were included for qualitative analysis and 14 articles for quantitative analysis (Figure 1).
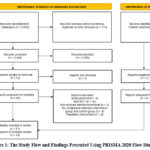 |
Figure 1: The Study Flow and Findings Presented Using PRISMA 2020 Flow Diagram10 |
Figure 2 shows that most of the risks of bias across all studies were low (n = 9) or unclear (n = 9). Meanwhile, Jadad’s study quality score indicates that all the studies were either fair (n = 9) or good (n = 12). Only eight studies employed both an assessor-blinded, randomised, controlled intervention design and outcomes, whereas the others either did not provide bias minimisation strategies or did not clarify this issue in their studies. Eighteen studies have complete outcome data or low attrition bias. However, all studies were considered essential for the present study.
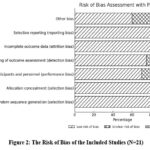 |
Figure 2: The Risk of Bias of the Included Studies (N=21) |
Characteristics of Included Studies
There were 21 studies on telenutrition services involving nine categories of intervention: weight loss intervention (n = 7), personalised nutrition and physical activity interventions (n = 3), diabetes care intervention (n = 3), metabolic syndrome (Mets) intervention (n = 2), bone health care intervention (n = 1), organ transplant intervention (n = 2), haematological cancer intervention (n = 1), kidney disease intervention (n = 1), and age-related macular degeneration (AMD). The three most common methods of telenutrition intervention are delivered by dietitians via telephone counselling (n = 8), video conferencing (an audio/visual approach) (n = 9), and interactive websites and platforms (including text messaging and email) (n = 4).
The duration of telephone counselling interventions varied considerably, ranging from three months18-21, four months22, six months23,24, and 12 months25 with the frequency of telephone calls being either weekly, fortnightly, or monthly. The longest call lasted for 30 minutes. Most interventions (n = 8) were conducted individually between a participant and dietitian via a video conference application such as Skype, Google Hangout, and FaceTime. In contrast, one study involved a virtual group with eight participants in each group26. On the other hand, the intervention via video conference was conducted for a minimum of two months27, three months26,28-31 four months32, six months33, and a maximum of 24 months34 The video counselling frequency ranged from weekly to monthly, with a duration of between 15 and 45 minutes per video call. One study provided a blended intervention with telehealth (11 x 15 minutes) and face-to-face (6 x 60 minutes) for exercise and dietary intake counselling33. Four studies provided internet-based health management platforms: websites, messenger, email, and computer chat35-38.
There was a multi-disciplinary approach used in the intervention, such as consultation by a dietitian with a medical doctor and physical activity expert/physiologist18,20,24,28,30,31. Telemonitoring devices such as wireless Bluetooth® devices and ‘smart’ scales were used to measure the body composition and physiological condition and track the physical activity of participants23,24,26,28,30,31. Most of the studies incorporated behavioural change techniques (health belief model, social cognitive theory model, and theory of planned behaviour) 19,22,23,25,27,28,30-33,35,36together with three key elements, which are health examination, nutrition education, and exercise education.
Several guidelines or protocols were used to guide the studies’ interventions, such as medical nutrition therapy (MNT) based on nutrition care practices (NCP), American Diabetes Association Standards (ADAs)19-21,25,34; Dietary Approaches to Stop Hypertension (DASH) diet25; WHO-recommended nutrition assessment38; and Australian Dietary Guidelines22,32. Most studies comprised an intervention group and a control group (usual or traditional care). Meanwhile, three studies included two intervention groups and a control group with no intervention provided27,33,35. Some of the control group participants received educational materials or workbooks, such as calorie and physical activity guidelines, a healthy lifestyle tracking calendar, and personalised dietary intake reports18,19,21,28,30-32.
Feasibility of Telenutrition
The feasibility of each implementation was assessed based on the following factors: the rate of recruitment, program attendance or adherence, intervention completion rate, and satisfaction during each implementation. The number of participants who agreed to take part in the study was divided by the total number of participants who attempted contact to get the recruitment rate39,40. Five studies successfully recruited 100% of the targeted sample population20,22,24,28,31,35. Meanwhile, other studies (n=8) ranged between 26% and 98% of recruitment rates. The completion of scheduled virtual consultations was measured as the attendance rate. At least 80% of completed consultations were considered feasible interventions39,40. Six studies were rated good to high adherence to the intervention, whereas 11 studies achieved >80% of the completed consultation intervention. In contrast, only three studies had low completion rates (<50%)27,34,35.
Eight studies18,19,22,24,27-29,32 reported on participants’ satisfaction as determined by the Likert scale or rating scale and/or qualitative interviews. All the studies showed a high satisfaction rate of 78% to 98.6% with the intervention program. Meanwhile, a study involving two intervention groups reported a higher proportion of coaching intervention (88% of tailoring and coaching) compared to non-coaching interventions (64% of tailoring only)27. Participants’ feedback summarised that the intervention programme was convenient, easy to use, informative (evidence-based), motivating, accountable, non-judgemental, and personalised18,22,27,28,32. However, some of the participants mentioned negative comments about the intervention programme, including a lack of personal contact and not being personalised enough27, while some of the participants had difficulty reporting or completing the tracking assessment on time28,32.
Effectiveness of Telenutrition
The effectiveness of telenutrition intervention was examined using meta-analysis, which included 14 studies with a total of 6,736 participants. The outcomes were divided into anthropometric measurements and physiological data for physiological conditions. The anthropometric data measured the changes in weight loss, BMI, and waist circumference. At the same time, the physiological condition involved clinical data such as triglycerides, total cholesterol, HDL cholesterol, glycated haemoglobin, fasting blood glucose, and blood pressure. Four studies recorded no statistical significance in the baseline characteristics between the intervention and control groups. Thirteen studies involved participants with BMI ≥ 27 kg/m2, while one study included normal weight to obese participants.
The Effectiveness of Telenutrition on Anthropometric Parameters
Statistically significant differences in body weight changes for the intervention group compared to usual care after a three- to 12-month telenutrition intervention were demonstrated by six studies23,24,26,30,31,35. Five studies recorded a significant weight reduction between -1.36 kg and -8.3 kg from baseline to post-intervention (12 weeks) in the intervention group19,26,29,31,35. One study stated a significant weight increment for kidney transplant patients +5.5kg with P=0.0328. Two studies show a significant BMI reduction of 0.7 kg/m2 and 0.3 kg/m2 in 12 weeks from baseline to post-intervention, respectively21,29, whereas four studies show a significant reduction in waist circumference from baseline to post-intervention between the intervention groups (3.5 cm, -3.0 cm, -2.0 cm, and -6.8 cm)19,21,29,36. The inclusion of diet and exercise with intervention resulted in a higher decrease in waist circumference by 2 cm (p < 0.001) and BMI by -0.36 kg/m2 (p < 0.001) in two years34. Generally, telenutrition, which was highlighted as an alternative to usual or traditional care, has significantly improved weight, BMI, and waist circumference.
Meta-analysis of the Effects of Telenutrition on Anthropometric Parameters
Ten studies involving 1,788 participants reported on the weight changes (Figure 3). P = 0.39; I2 = 6% showed low heterogeneity across the studies. Thus, a fixed effect model was used to calculate the mean effect size. Mean difference (MD) was used as the same measurement scale for all involved studies. The weight changes between the telenutrition and normal care groups were found to be significantly different, according to the data (MD = -2.36; 95% CI = -3.91, -0.81; Z = 2.99; P = 0.003).
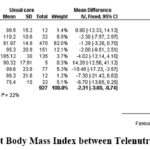 |
Figure 3: Forest Plot Body Mass Index between Telenutrition and Usual Care |
Nine studies involving 2,046 participants reported BMI findings (Figure 4). P = 0.22; I2 = 25% showed low heterogeneity across the studies. The results revealed statistically significant differences in BMI values between the telenutrition and usual care groups (MD = -0.10; 95% CI = -0.19, -0.00; Z = 2.06; P = 0.04).
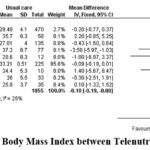 |
Figure 4: Forest Plot Body Mass Index between Telenutrition and Usual Care |
Seven studies involving 1,027 participants reported waist circumference (Figure 5). P = 0.17; I2 = 34% showed moderate heterogeneity across the studies. The results showed statistically significant differences in waist circumference between the telenutrition and usual care groups. (MD = -3.53; 95% CI = -4.31, -2.74; Z = 8.82; P < 0.00001).
 |
Figure 5: Forest Plot on Waist Circumference between Telenutrition and Usual Care |
The Effectiveness of Telenutrition on Biochemical Data
All studies show no significant difference in biochemical data between control and intervention groups. However, only one study showed a significant reduction in fasting blood glucose between the control and intervention groups after three months of intervention36. Triglycerides and total cholesterol significantly decreased in the intervention group from baseline to post-intervention in three and six months of intervention: -26.1 mg/dl (p = 0.01), -55.1 mg/dl (p = 0.05), -13 mg/dl (p = 0.038), and -26.9 mg/dl (p = 0.01)21,24. A significant improvement in the composite optimal diabetes care measure from baseline to follow-up in 12 months but no statistically significant difference in HbA1c values was found in the intervention group25. There was no statistical difference in HbA1c values between the intervention and control groups23. HbA1c values within telephone counselling groups, however, decreased significantly (P = 0.027) by means 95% CI, from 7.3% (7.0, 7.6) at baseline to 7.1% (6.9, 7.3) at follow-up. The effectiveness of telenutrition intervention in measuring biochemical data, particularly in glycaemic control, blood pressure, and cholesterol levels, is limited when compared to usual or traditional care.
Meta-analysis of the Effects of Telenutrition on Biochemical Parameters.
Four studies involving 286 participants reported on the triglyceride levels (Figure 6). P = 0.81; I2 = 0% showed no heterogeneity across the studies. The results showed that there were statistically significant differences in triglyceride levels between the telenutrition and usual care groups (MD = -17.12; 95% CI = -27.90, -6.33; Z = 3.11; P = 0.002).
 |
Figure 6: Forest Plot on Triglyceride Levels between Telenutrition and Usual Care |
Six biochemical parameters involving total cholesterol, HDL-cholesterol, hemoglobin A1c, fasting blood glucose, diastolic blood pressure, and systolic blood pressure showed no significant different between telenutrition group and usual care group (supplementary). Two studies involving 101 participants reported on the total cholesterol levels. P = 0.20; I2 = 38% showed moderate heterogeneity across the studies. The results favour the normal care, as indicated by the diamond shape, which is situated to the right of the line of no effect (the vertical line at mean difference). This means that traditional care had a lower risk or better outcome than the telenutrition group41. Thus, the results favour usual care with no statistically significant differences in total cholesterol levels (MD = 9.27; 95% CI = -3.98, -22.52; Z = 1.37; P = 0.17). Four studies involving 286 participants reported on the HDL-cholesterol levels. P = 0.72; I2 = 0% showed no heterogeneity across the studies. The results favour usual care, showing no statistically significant differences in HDL-cholesterol levels (MD = 2.26; 95% CI = -2.25, 4.77; Z = 1.76; P = 0.08). Three studies involving 420 participants reported on haemoglobin A1c (HbA1c) values. P = 0.28; I2 = 0% showed no heterogeneity across the studies. The results favour telenutrition, showing no statistically significant differences in HbA1c values (MD = -0.15; 95% CI = -0.41, 0.12; Z = 1.07; P = 0.28). Four studies involving 286 participants reported on fasting blood glucose levels. P = 0.71; I2 = 0% showed no heterogeneity across the studies. The results revealed no statistically significant differences in fasting blood glucose levels between the telenutrition and usual care groups (MD = -0.64; 95% CI = -6.02, 4.73; Z = 0.23; P = 0.81). Four studies involving 286 participants reported on the diastolic blood pressure. P = 0.19; I2 = 37% showed moderate heterogeneity across the studies. The results favour telenutrition, demonstrating no significant differences in diastolic blood pressure (MD = -1.83; 95% CI = -4.39, 0.73; Z = 1.40; P = 0.16). Four studies involving 286 participants reported on the systolic blood pressure. P = 0.94; I2 = 0% showed no heterogeneity across the studies. With no significant differences in systolic blood pressure (MD = -3.46; 95% CI = -7.05, 0.13; Z = 1.89; P = 0.06), the findings leaned toward telenutrition.
Subgroup Analysis
Subgroup analysis was performed for more in-depth comparisons of subgroups with the weight change in terms of type of intervention, duration of intervention, and total number of participants (Table 1). The summary findings show that telephone-based intervention significantly decreased body weight. The duration of intervention, < 6 months, and the number of participants of < 100, significantly (p = 0.04) reduced the body weight between the telenutrition intervention group and the control group.
Table 1: Subgroup Analysis for Weight Changes (N=10)
|
Subgroup |
N | Pooled outcomes | Heterogeneity | |||
|
Mean difference (95% CI) |
P | Q |
I2 |
|||
| Type of intervention |
|
|||||
|
Telephone |
3 | -5.38 (-9.40, -1.36) | 0.009* | 4.37 | 31 | 0.22 |
| Videoconference | 4 | -2.38 (-6.52, 1.77) | 0.26 | 1.43 | 0 |
0.84 |
|
Web-based (internet) |
2 | -1.44 (-3.38, 0.49) | 0.14 | 0.41 | 0 | 0.52 |
| Length of intervention |
|
|||||
|
< 6months |
6 | -1.82 (-3.56, -0.08) | 0.04* | 3.66 | 0 | 0.72 |
| ≥ 6months | 3 | -5.10 (-10.31, 0.12) | 0.06 | 4.06 | 51 |
0.13 |
|
Total participants |
||||||
|
< 100 |
5 | -3.51 (-7.07, 0.05) | 0.05* | 2.52 | 0 | 0.77 |
| ≥ 100 | 4 | -3.41 (-6.91, 0.09) | 0.06 | 6.52 | 54 |
0.09 |
N= number of studies, Q= Chi2, I2=Heterogeneity
*Significant difference between the intervention group and control group
Publication Bias
Figure 7 presents an evaluation of publication bias, incorporating effect size estimates from individual studies and a precision measure. The observed studies involved are represented by the shapes of scattered objects in the funnel plot. The standard error moves toward zero where there are larger studies as the studies, clustered closely near the top of the plot. The Egger’s test42 showed there was no significant evidence of publication bias in weight changes (t = -0.14, p = 0.45), BMI (t = -0.87, p = 0.42), waist circumference (t = -0.39, p = 0.46), triglyceride (t = -0.30, p = 0.54), HDL-cholesterol (t = 0.21, p = 0.94), HbA1c (t = -0.09, p = 0.62), fasting blood glucose (t = -0.03, p = 0.83), diastolic blood pressure (t = -0.12, p = 0.58), systolic blood pressure (t = -0.22, p = 0.59). The certainty in the body of evidence (GRADE) indicated that two study outcomes were low, five studies were moderate, and three studies were high.
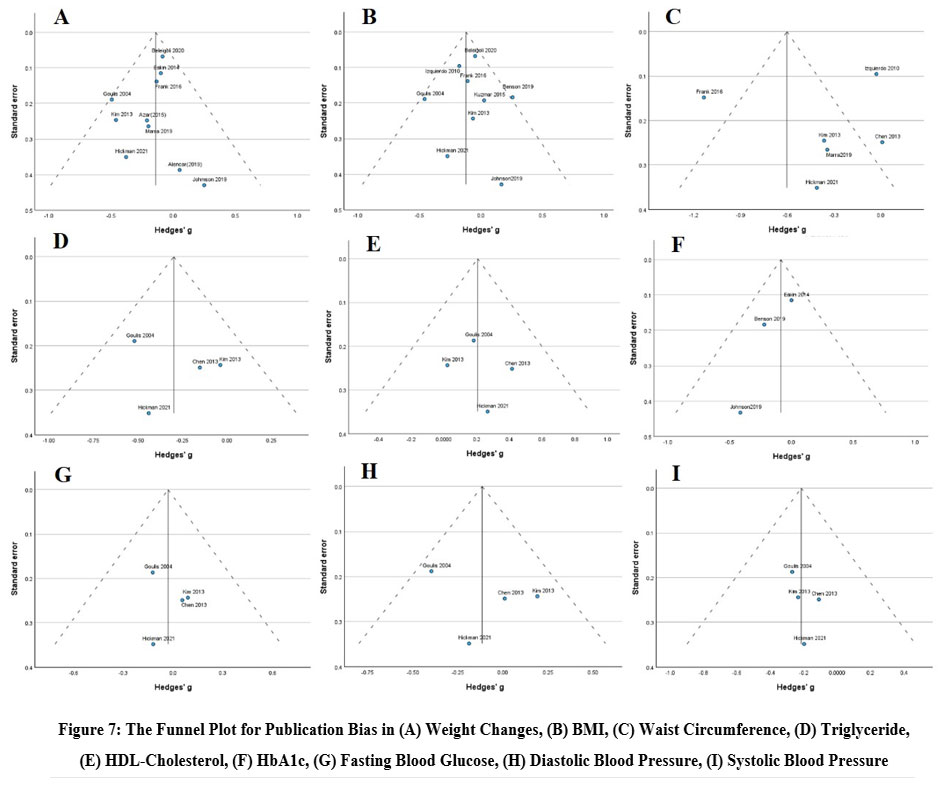 |
Figure 7: The Funnel Plot for Publication Bias in (A) Weight Changes, (B) BMI, (C) Waist Circumference, (D) Triglyceride, (E) HDL-Cholesterol, (F) HbA1c, (G) Fasting Blood Glucose, (H) Diastolic Blood Pressure, (I) Systolic Blood Pressure |
Discussion
The important factors contributing to successful telenutrition services include feasibility and effectiveness. Feasibility is based on patients’ active engagement in treatment, frequent weight monitoring, motivation, health care surveillance, and personalised individual feedback. This review demonstrated that telenutrition interventions are feasible based on excellent recruitment, adherence, completion, and satisfaction rates.
The important factors contributing to a successful intervention are patients’ active engagement in the treatment; frequent weight monitoring; motivation; healthcare surveillance; and personalised individual feedback24. Participants withdrew due to illness, school or work schedule conflicts, and technical issues. Meanwhile, failure to lose weight and reach personal weight targets was due to a lack of motivation38. Poor usability of the intervention, a lack of interest in it, and mental and physical health problems led to higher dropout rates. The reason was that participants felt burdened; personalised feedback was not based on their preferences; and the usability of the computer tailoring was poor43.
A recent study conducted, involved motivational and educational online tools promoting lifestyle and eating behaviour changes, diet therapy plans, and individualised nutritional counselling to improve patients’ health44. Participants are more motivated to change their behaviour when self-selection is used in behaviour-based trials than those who do not participate19. According to Beleigoli (2020), telenutrition via a web-based platform results in a more substantial weight loss, a rise in fruit and vegetable consumption, and a drop in the consumption of ultra-processed foods than minimal intervention. Most overweight patients chose telenutrition for their intervention programme because it provides a flexible, comfortable, and cost-effective alternative to traditional methods38. A comprehensive approach through extensive lifestyle education, patient education, behavioural changes, regular follow-up with dietitians, an easy platform, adequate equipment and technologies, and personalised sessions for diet and exercise support are highly preferable by individuals or groups.
To adequately familiarise patients with the technology, it is crucial to ensure self-assurance and unsupervised learning. This also applies to teaching clinical staff how to troubleshoot technical connection issues in real time29. A suggestion to increase participant compliance is to provide an automatic online system for participants to record and upload daily dietary intake and physical activities. Thus, it would be more convenient and efficient for health management experts to provide personalised feedback based on their records36.
A combination of several key elements, including telenutrition coaching, effectively reduces body weight significantly in obese adults (>5%); it also promotes compliance to dietary plans (e.g., low-calorie diet with low glycaemic index), physical activity compliance, and behavioural changes24,31. The availability of self-monitoring Bluetooth wireless devices and personalised feedback also promotes long-term engagement in weight loss programmes31. A recent retrospective study in Brazil found that weight, BMI, waist circumference, waist-to-height ratio, body fat, and lean body mass all decreased significantly, suggesting the effectiveness of telenutrition intervention in a 6-month nutrition education program.
Telemedicine interventions for managing diabetes during the COVID-19 pandemic resulted in notable improvements in glycemic control, including lower HbA1c values and improved glucose control. These results demonstrate how telemedicine systems, such as personalized dietary advice and ongoing glucose monitoring, can help patients achieve improved health outcomes while providing flexibility and convenience45. For instance, the effects of a smartphone-based intervention for individuals with type 2 diabetes were investigated in the TRIGGER research46. In comparison to the control group, participants who got personalized nutritional feedback, regular self-monitoring prompts, and targeted instructional messages showed better HbA1c levels, healthier eating habits, and more satisfaction with diabetes care. This demonstrates how patient-centered mobile health technologies can improve chronic disease management efficacy and engagement.
Strengths and Limitations
The present study’s strength lies in the meta-analysis findings that demonstrate the feasibility and effectiveness of telenutrition services. The feasibility outcome showed a high satisfaction rate ranging from 78% to 98.6%, indicating that participants were interested in receiving telenutrition intervention. The meta-analysis assessed the most common anthropometric and biochemical data to identify physiological outcomes that could potentially improve patients’ health conditions. A sub-group analysis calculated the BMI outcome, which indicated the type of intervention, length of intervention, and total number of participants, thereby enhancing the effectiveness of telenutrition services.
This review’s main limitation is that the results may be influenced by variations in participant baseline characteristics for each RCT sample population, including anthropometric measurements and biochemical data. However, most studies show no significant baseline difference between the intervention group and the usual care group. Moreover, the meta-analysis included fewer than ten studies for the individual outcomes of waist circumference, total cholesterol, triglyceride, HDL-cholesterol, HbA1c, fasting blood glucose, and blood pressure. Future research should comprise more studies on these outcomes to strengthen the evidence regarding the effectiveness of telenutrition findings.
Conclusion
This review of telenutrition services highlights the key factors that contribute to their success, primarily focusing on feasibility and effectiveness. Feasibility was demonstrated through active patient engagement, regular weight monitoring, motivation, healthcare surveillance, and personalised feedback, which led to high recruitment, adherence, and satisfaction rates. However, dropout rates were linked to factors such as poor usability, technical issues, and lack of motivation, as reported in various studies. Overall, telenutrition interventions were proven to be effective in promoting weight loss, reducing waist circumferences, and improving triglyceride level, particularly when comprehensive tools and personalised support were provided. More research is needed to assess the efficacy of telenutrition services in physiological parameters such HbA1c levels, lipid profile, and blood pressure.
Acknowledgement
We express our sincere gratitude to our research team, whose dedication and collaborative efforts have been instrumental in the successful completion of this study.
Funding Sources
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicts of Interest
The authors declare no conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval.
Informed Consent Statement
This study did not involve human participants, and therefore, informed consent was not required.
Clinical Trial Registration
This research does not involve any clinical trials.
Permission to reproduce material from sources
Not applicable
Author Contributions
- Nur Liyana Hasnaa Mohd Daud : Literature search
- Nur Liyana Hasnaa Mohd Daud, Nor Azwani Mohd Shukri: Original Draft Preparation
- Nur Liyana Hasnaa Mohd Daud, Nor Azwani Mohd Shukri, Noraishah Mohamed Nor: Conceptualisation; Data Analysis
- Nor Azwani Mohd Shukri, Noraishah Mohamed Nor, Wan Azdie Mohd Abu Bakar, Nurul Hazirah Jaafar: Review and Editing; Supervision
References
- Reynolds R, Dennis S, Hasan I, Slewa J, Chen W, Tian D, Bobba S, Zwar N. A Systematic Review of Chronic Disease Management Interventions in Primary Care. BMC Fam Pract. 2018;19(1):11. doi:10.1186/s12875-017-0692-3
CrossRef - Khaw WF, Chan YM, Nasaruddin NH, Alias N, Tan L, Ganapathy S.S. Malaysian Burden of Disease: Years of Life Lost Due to Premature Deaths. BMC Public Health. 2023;23(1):1383. doi:10.1186/s12889-023-16309-z
CrossRef - National Institutes of Health, Ministry of Health Malaysia. National Health and Morbidity Survey (NHMS) 2023: Vol. I: NCDs—Non-Communicable Diseases: Risk Factors and other Health Problems. 2023.
- Budreviciute A, Damiati S, Sabir D. K, Onder K, Schuller-Goetzburg P, Plakys G, Katileviciute A, Khoja S, Kodzius R. Management and Prevention Strategies for Non-communicable Diseases (NCDs) and Their Risk Factors. Front Public Health. 2020. https://www.frontiersin.org/article/10.3389/fpubh.2020.574111
CrossRef - World Health Organization. The Impact of the COVID-19 Pandemic on Non-communicable Disease Resources and Services: Results of a Rapid Assessment. Geneva. https://www.who.int/publications/i/item/WPR-DSE-2020-032. November 13, 2020
- Saleh Z. T, Elshatarat R. A, Elhefnawy K. A, Elneblawi H. N, Abu Raddaha A. H, Al-Za’areer M. S, Mofdy Almarwani A, Alzahrani N. S, Aqel A. A, Shawashi T. O, Tayeh M. Effect of a Home-based Mobile Health App Intervention on Physical Activity Levels in Patients with Heart Failure: A Randomized Controlled Trial. J Cardiovasc Nurs. 2023;38(2):128-139. doi:10.1097/JCN.0000000000000911
CrossRef - Gokalp H, de Folter J, Verma V, Fursse J, Jones R, Clarke M. Integrated Telehealth and Telecare for Monitoring Frail Elderly with Chronic Disease. Telemed J E Health. 2018;24(12):940-957. doi:10.1089/tmj.2017.0322
CrossRef - Clarke M, Fursse J, Brown-Connolly N. E, Sharma U, Jones R. Evaluation of the National Health Service (NHS) Direct Pilot Telehealth Program: Cost-Effectiveness Analysis. Telemed J E Health. 2018;24(1):67-76. doi:10.1089/tmj.2016.0280
CrossRef - Page M. J, McKenzie J. E, Bossuyt P. M, Boutron I, Hoffmann T. C, Mulrow C. D, Shamseer L, Tetzlaff J. M, Akl E. A, Brennan S. E, Chou R, Glanville J, Grimshaw J. M, Hróbjartsson A, Lalu M. M, Li T, Loder E. W, Mayo-Wilson E, McDonald S, McGuinness L. A, Stewart L. A, Thomas J, Tricco A. C, Welch V. A, Whiting P, Moher D. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ. 2021;372:71. doi:10.1136/bmj.n71
CrossRef - Daud N. L. H. M, Nor N. M, Jaafar N. H, Bakar W. A. M. A, Shukri N. A. M. The Feasibility and Effectiveness of Telenutrition for Remote Dietary Consultation: A Systematic Review and Meta-analysis Protocol. Malays J of Med and Health Sci. 2023;19(9):337-342. doi:10.47836/mjmhs.19.s9.46
CrossRef - Higgins J. P, Altman D. G, Gøtzsche P. C, Jüni P, Moher D, Oxman A. D, Savović J, Schulz K. F, Weeks L, Sterne J. A. C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ. 2011;343:5928. doi:10.1136/bmj.d5928
CrossRef - Cochrane Collaboration. Review Manager (RevMan) [Computer Program]. Copenhagen. 2011.
- Jadad A. R, Moore R. A, Carroll D, Jenkinson C, Reynolds D. J, Gavaghan D. J, McQuay H. J. Assessing the Quality of Reports of Randomized Clinical Trials: Is Blinding Necessary? Control Clin Trials. 1996;17(1):1-12. doi:10.1016/0197-2456(95)00134-4
CrossRef - Guyatt, G. H., Oxman, A. D., Kunz, R., Brozek, J., Alonso-Coello, P., Rind, D., … & Schünemann, H. J. (2011). GRADE guidelines: 6. Rating the quality of evidence—imprecision. Journal of Clinical Epidemiology, 64(12), 1283-1293. https://doi.org/10.1016/ j.jclinepi.2011.01.012
CrossRef - Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, Britten N, Roen K, Duffy S. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: A Product from the ESRC Methods Programme. 2006.
- Haidich A. B. Meta-analysis in Medical Research. Hippokratia. 2010;14(1):29-37.
- Sterne J. A. C, Sutton A. J, Ioannidis J. P. A, Terrin N, Jones D. R, Lau J, Carpenter J, Rücker G, Harbord R. M, Schmid C. H, Tetzlaff J, Deeks J. J, Peters J, Macaskill P, Schwarzer G, Duval S, Altman D. G, Moher D, Higgins J. P. T. Recommendations for Examining and Interpreting Funnel Plot Asymmetry in Meta-Analyses of Randomised Controlled Trials. BMJ. 2011;343:4002. doi:10.1136/bmj.d4002
CrossRef - Kelly J. T, Conley M, Hoffmann T, Craig J. C, Tong A, Reidlinger D. P, Reeves M. M, Howard K, Krishnasamy R, Kurtkoti J, Palmer S. C, Johnson D. W, Campbell K. L. A Coaching Program to Improve Dietary Intake of Patients with CKD: ENTICE-CKD. Clin J Am Soc Nephrol. 2020;15(3):330-340. doi:10.2215/CJN.12341019
CrossRef - Ventura Marra M, Lilly C. L, Nelson K. R, Woofter D. R, Malone J. A. Pilot Randomized Controlled Trial of a Telenutrition Weight Loss Intervention in Middle-Aged and Older Men with Multiple Risk Factors for Cardiovascular Disease. Nutrients. 2019;11(2):229. doi:10.3390/nu11020229
CrossRef - Hung Y. C, Bauer J. D, Horsely P, Coll J, Bashford J, Isenring E. A. Telephone-delivered Nutrition and Exercise Counselling After Auto-SCT: A Pilot, Randomised Controlled Trial. Bone Marrow Transplant. 2014;49(6):786-792. doi:10.1038/bmt.2014.52
CrossRef - Kim J, Bea W, Lee K, Han J, Kim S, Kim M, Na W, Sohn C. Effect of the Telephone-Delivered Nutrition Education on Dietary Intake and Biochemical Parameters in Subjects with Metabolic Syndrome. Clin Nutr Res. 2013;2(2):115-124. doi: 10.7762/cnr.2013.2.2.115
CrossRef - Tang D, Mitchell P, Liew G, Burlutsky G, Flood V. M, Gopinath B. Telephone-Delivered Dietary Intervention in Patients with Age-Related Macular Degeneration: 3-Month Post-Intervention Findings of a Randomised Controlled Trial. Nutrients. 2020;12(10):3083. doi:10.3390/nu12103083
CrossRef - Eakin E. G, Winkler E. A, Dunstan D. W, Healy G. N, Owen N, Marshall A. M, Graves N, Reeves M. M. Living Well with Diabetes: 24-Month Outcomes from a Randomized Trial of Telephone-Delivered Weight Loss and Physical Activity Intervention to Improve Glycemic Control. Diabetes Care. 2014;37(8):2177-2185. doi:10.2337/dc13-2427
CrossRef - Goulis D. G, Giaglis G. D, Boren S. A, Lekka I, Bontis E, Balas E. A, Maglaveras N, Avramid A. Effectiveness of Home-centered Care Through Telemedicine Applications for Overweight and Obese Patients: A Randomized Controlled Trial. Int J Obes Relat Metab Disord. 2004;28(11):1391-1398. doi:10.1038/sj.ijo.0802773
CrossRef - Benson G. A, Sidebottom A, Hayes J, Miedema M. D, Boucher J, Vacquier M, Sillah A, Gamam S, VanWormer J. J. Impact of ENHANCED (diEtitiaNs Helping pAtieNts CarE for Diabetes) Telemedicine Randomized Controlled Trial on Diabetes Optimal Care Outcomes in Patients with Type 2 Diabetes. J Acad Nutr Diet. 2019;119(4):585-598. doi:10.1016/j.jand.2018.11.013
CrossRef - Azar K. M, Aurora M, Wang E. J, Muzaffar A, Pressman A, Palaniappan L. P. Virtual Small Groups for Weight Management: An Innovative Delivery Mechanism for Evidence-Based Lifestyle Interventions Among Obese Men. Transl Behav Med. 2015;5(1):37-44. doi:10.1007/s13142-014-0296-6
CrossRef - Alley S, Jennings C, Plotnikoff R. C, Vandelanotte C. Web-Based Video-Coaching to Assist an Automated Computer-Tailored Physical Activity Intervention for Inactive Adults: A Randomized Controlled Trial. J Med Internet Res. 2016;18(8):223. doi:10.2196/jmir.5664
CrossRef - Gibson C. A, Gupta A, Greene J. L, Lee J, Mount R. R, Sullivan D. K. Feasibility and Acceptability of a Televideo Physical Activity and Nutrition Program for Recent Kidney Transplant Recipients. Pilot Feasibility Stud. 2020;6(1):126. doi:10.1186/s40814-020-00672-
CrossRef - Hickman I. J, Hannigan A. K, Johnston H. E, Elvin-Walsh L, Mayr H. L, Staudacher H. M, Barnett A, Stoney R, Salisbury C, Jarrett M, Reeves M. M, Coombes J. S, Campbell K. L, Keating S. E, Macdonald G. A. Telehealth-delivered, Cardioprotective Diet and Exercise Program for Liver Transplant Recipients: A Randomized Feasibility Study. Transplant Direct. 2021;7(3):667. doi:10.1097/TXD.0000000000001118
CrossRef - Johnson K. E, Alencar M. K, Coakley K. E, Swift D. L, Cole N. H, Mermier C. M, Kravitz L, Amorim F. T, Gibson A. L. Telemedicine-Based Health Coaching Is Effective for Inducing Weight Loss and Improving Metabolic Markers. Telemed J E Health. 2019;25(2):85-92. doi:10.1089/tmj.2018.0002
CrossRef - Alencar M. K, Johnson K, Mullur R, Gray V, Gutierrez E, Korosteleva O. The efficacy of A Telemedicine-based Weight Loss Program with Video Conference Health Coaching Support. J Telemed Telecare. 2019;25(3):151-157. doi:10.1177/1357633X17745471
CrossRef - Rollo M. E, Haslam R. L, Collins C. E. Impact on Dietary Intake of Two Levels of Technology-Assisted Personalized Nutrition: A Randomized Trial. Nutrients. 2020;12(11):3334.
CrossRef - van den Helder J, Verlaan S, Tieland M, Scholten J, Mehra S, Visser B, Kröse B. J. A, Engelbert R. H. H, Weijs P. J. M. Digitally Supported Dietary Protein Counseling Changes Dietary Protein Intake, Sources, and Distribution in Community-Dwelling Older Adults. Nutrients. 2021;13(2):502. doi: 10.3390/nu13020502
CrossRef - Izquierdo R, Lagua C. T, Meyer S, Ploutz-Snyder R. J, Palmas W, Eimicke J. P, Kong J, Teresi J. A, Shea S, Weinstock R. S. Telemedicine Intervention Effects on Waist Circumference and Body Mass Index in The IDEATel Project. Diabetes Technol Ther. 2010;12(3):213-220. doi:10.1089/dia.2009.0102
CrossRef - Beleigoli A, Andrade A. Q, Diniz M. D. F, Ribeiro A. L. Personalized Web-Based Weight Loss Behavior Change Program with and Without Dietitian Online Coaching for Adults with Overweight and Obesity: Randomized Controlled Trial. J Med Internet Res. 2020;22(11):17494. doi:10.2196/17494
CrossRef - Chen Y. C, Tsao L. I, Huang C. H, Yu Y. Y, Liu I. L, Jou H. J. An Internet-based Health Management Platform May Effectively Reduce the Risk Factors of Metabolic Syndrome Among Career Women. Taiwan J Obstet Gynecol. 2013;52(2):215-221. doi:10.1016/j.tjog.2013.04.011
CrossRef - Frank L. L, McCarthy M. S. Telehealth Coaching: Impact on Dietary and Physical Activity Contributions to Bone Health During a Military Deployment. Mil Med. 2016;181(5 Suppl):191-198. doi:10.7205/MILMED-D-15-00159
CrossRef - Kuzmar I. E, Cortés-Castell E, Rizo M. Effectiveness of Telenutrition in A Women’s Weight Loss Program. PeerJ. 2015;3:748. doi:10.7717/peerj.748
CrossRef - Lima D. P, Gomes V. C, Viana Júnior A. B, Carvalho de Assis F. M, Oliveira P. H. A, Cunha L. C. V, Braga I. C, Marques M. L. S, Assunção J. D. S, Damasceno A. L. L, Barbosa A. L. G, Moreira A. H, Rocha M. E. Q. A, Porto M. E. M. P, Chaves E. C. B, de Oliveira L. M, Roriz Filho J. de Sá, Sobreira Neto M. A, Neto P. B. Telehealth for Parkinson Disease Patients During The COVID-19 Pandemic: The TeleParkinson Study. Telesaúde para pacientes com doença de Parkinson durante a pandemia de COVID-19: o estudo TeleParkinson. Arq Neuropsiquiatr. 2022;80(10):1026-1035. doi:10.1055/s-0042-1758751
CrossRef - Peniche P, Pinto A, Ribeiro R, Martins J, Faria C. Recruitment, Retention, Attendance, and Adherence of a Randomized Controlled Trial to Evaluate the Effects of Task-Specific Training with Individuals Post Stroke. Fisioterapia e Pesquisa. 2022;29:22-28. doi:10.1590/1809-2950/20008529012022en
CrossRef - Ahn E, Kang H. Introduction to Systematic Review and Meta-analysis. Korean J Anesthesiol. 2018;71(2):103-112. doi:10.4097/kjae.2018.71.2.103
CrossRef - Egger M, Smith G. D, Schneider M, Minder C. Bias in Meta-analysis Detected by a Simple, Graphical Test. BMJ. 1997;315(7109):629-634. doi:10.1136/bmj.315.7109.629
CrossRef - Opie J. E, Vuong A, Welsh E. T, Esler T. B, Khan U. R, Khalil H. Outcomes of Best-Practice Guided Digital Mental Health Interventions for Youth and Young Adults with Emerging Symptoms: Part II. A Systematic Review of User Experience Outcomes. Clin Child Fam Psychol Rev. 2024;27(2):476-508. doi:10.1007/s10567-024-00468-5
CrossRef - Piovacari S. M. F., Bisogni G. T. B., Jensen N. S. O, Lottenberg A. M. Impact of a Telenutrition Intervention on Body Composition and Eating Behaviour Changes in Individuals Living with Excess Weight. Austin J Public Health Epidemiol. 2023;10(3): 1151.
CrossRef - Sotomayor F, Hernandez R, Malek R, Parimi N, Spanakis E. K. The Effect of Telemedicine in Glycemic Control in Adult Patients with Diabetes during the COVID-19 Era—A Systematic Review. J of Clin Med. 2023; 12(17):5673. https://doi.org/10.3390/jcm12175673
CrossRef - Boels A. M., Vos R. C., Dijkhorst-Oei L. T., Rutten G. E. H. M. Effectiveness of diabetes self-management education and support via a smartphone application in insulin-treated patients with type 2 diabetes: Results of a randomized controlled trial (TRIGGER study). BMJ Open Diabetes Res Care. 2019;7(1):e000981. doi:10.1136/bmjdrc-2019-000981.
CrossRef

This work is licensed under a Creative Commons Attribution 4.0 International License.






