
Introduction
The global rise of overweight and obesity is a pressing health concern which can increases the risk of cardiovascular diseases (CVDs). According to the World Health Organization (WHO), obesity has tripled since 1975.1 Globally, over 2.5 billion adults aged 18years and older were overweight, and 890 million were obese (43% of men and 44% of women) in 2022.2 In Saudi Arabia, the situation is even more concerning. In 2016 WHO reported that the obesity in KSA is reached 20.2%, and overweight 38.2% and were higher in women (21.4%) than men (19.2%).3 Various strategies, including dietary modifications, increased physical activity, medication, and surgical interventions, have been proposed to address this growing public health issue.4 Although there is general agreement on weight loss strategies, specific approaches, such as diet plans, exercise routines, and medications, can vary.5 Recently, high-fat, low-carb ketogenic (keto) diets have gained significant interest. According to McGaugh and Barthel (2022), the keto diet was the most searched diet on Google in the US in 2022, with over 25 million searches. 6 The keto diet involves drastically reducing carbohydrates to less than 50 grams per day and replacing them with a high proportion of fats and a moderate amount of protein.7 This diet induces a metabolic state called ketosis in which the body shifts from using glucose as its primary source of energy to using ketones, which are produced from the breakdown of fats. 8 This shift occurs because a low intake of carbohydrates significantly reduces blood glucose and insulin levels, prompting the body to utilize stored fat for energy. 9 9 In a review study emphasized that ketogenic diets can lead to significant reductions in body weight, BMI, and waist circumference as well as improvements in lipid profiles, including reductions in triglycerides and increases in HDL cholesterol.10 These changes are crucial because abdominal obesity is a major risk factor for CVD. 10,11 Although the Saudi Ministry of Health (2020) acknowledged the effectiveness of the keto diet for treating epilepsy with medical supervision, worldwide, research on its use for weight loss and other health benefits is ongoing. The WHO emphasizes diversifying food choices to meet the body’s needs and prevent chronic diseases. 12 The aim of the present study was to compare the effects of a high-fat ketogenic diet (HFKD) and a low-fat diet (LFD) on weight loss, lipid profiles, and CVD risk factors in overweight and obese women.
Materials and Methods
Study design and participates
The study was a 12-week randomized controlled trial with a single-blind design, involving 28 healthy overweight or obese women who were randomly assigned to either the HFKD group (n = 14) or the LFD group (n = 14). The randomization schedules were created using a centrally controlled, computer-generated random number system accessible via the internet, and were concealed until an eligible participant was ready for enrollment13. All study participants were recruited from Al-Ahsa Province, Saudi Arabia from January to April 2023. The inclusion criteria were an age of 18 and 40 years and BMI (the weight in kilograms divided by the square of the height in meters) between 25 and 34.6 kg/m² and fat percentages between 30% and 50%, and not suffering from chronic diseases. The exclusion criteria included people with chronic diseases, pregnancy, lactation, treatment for high blood lipids, individuals who following a weight loss program or took weight loss medication and/or use of dietary supplements. The study was approved by the King Faisal University Ethics Committee (KFU – REC – 2021 – OCT EA00089) and registered at (https://clinicaltrials.gov) (ID: NCT05811702). The study was adhered to the Declaration of Helsinki guidelines. All participants provided informed consent before enrollment in this study (Figure 1).
 |
Figure 1: Flow of the study participants through the intervention. |
Diet interventions
Participants in the HFKD group (n = 14) were designed to follow a high fat diet with 70% fat, 10% carbohydrates and 20% protein from total energy intake (according to their daily calorie requirements for 12 weeks.14,15 The LFD group (n = 14) were designed to follow a low-fat diet with 20% fat, 55% carbohydrates and 25% protein from total energy intake daily for 12 weeks (Figure 2). Both diets were equal in terms of total energy intake but differed with regard to macronutrient content (fat, carbohydrates and protein). The LFD group was consumed various carbohydrates in their daily meals however, avoiding food high in sugar, white bread, pastries, sugary drinks. Saturated fat was kept below 10% in both diets and no supplements, artificial sweeteners, or other food and drink items were allowed for both group diets. All the participants received weekly meal plans that included breakfast, lunch, dinner, and snacks and counselling sessions with dietitian with advice during the 12-weeks. The education session foe meal plans and supported participants provide by the dietitian for all participants. The daily energy requirement for each participant was based on the basal metabolic rate, which was calculated using the modified Harris–Benedict equation and multiplied by an individua.16 All the participants were providing photograph and lists food recorded that participant ate daily in different diet groups.17 All participants were required to wear smart watch during the 12 weeks of following the diets to record their regular physical activity. Participant were advice to maintain a physical activity level of 8,000–10,000 steps per day throughout the 12-week intervention period. For the HFKD group, ketone concentrations in urine were measured using reagent slides to ensure ketosis.18
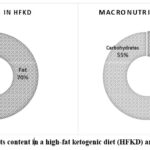 |
Figure 2: Macronutrients content in a high-fat ketogenic diet (HFKD) and a low-fat diet (LFD). |
Anthropometric measurements and blood samples
The primary outcome on this study was change in body weight, body fat and BMI. The secondary outcomes including lipid prefile (Total cholesterol, LDL, HDL and triglycerides), glucose levels, and blood pressure. Anthropometric measurements were conducted in the early morning, between 8:00 a.m. and 11:00 a.m. after an overnight fast of 8–12 hours. The body weight, and fat percentages, of all participants were obtained weekly using InBody (body composition analyzer) 170 device (Biospace, Seoul, South Korea) at the nutrition clinic at King Faisal University. Blood pressure was measured weekly, and participants were rested for 30 min, and the mean of triplicate measurements was recorded with an OMRON-M6 automatic digital (HEM-7211-E8) Comfort Upper-Arm Blood Pressure Monitor. Blood samples were collected, after participants had fasted for 8 hours to measure plasma glucose, total cholesterol, triglycerides, LDL, HDL, HbA1c, and urinary albumin (Analyzer Vitros, 5600, Ortho Clinical Diagnostics) at the health center at King Faisal University. Blood samples were analyzed at the baseline and at 12 weeks.
Statistical analysis
Power calculations were conducted based on changes in body weight, BMI, and body fat percentage from a previous study.19 The required sample size was estimated using a t-test for the two groups with the G*Power program. Data were expressed as mean ± standard deviation (SD) and percentages to describe and compare responses among individuals. The normality of the data was assessed before analysis. Paired t-tests and chi-square tests were employed to compare mean values at baseline and after 12 weeks. An independent samples t-test was used to compare the effects of the diets after 12 weeks. IBM’s Statistical Package for Social Sciences (SPSS) version 23 was used for analysis, with statistical significance set at p < 0.05.
Results
Characteristics of the participants
The characteristics of the study population are summarized in Table 1. A total of 28 eligible overweight/ obsess participants were randomly assigned to the HFKD (n=14) and LFD (n=14). The participants were women aged 18–40 years with a BMI of 25–34.6 kg/m2 and a fat percentage of 30–50%. The participants were in good health and free from any food allergies that could impact their dietary adherence. There were no significant differences between two group in the participants’ baseline characteristics, anthropometric data, or laboratory measurements. The average age, weight, height, BMI, and waist circumference values were show in Table 1. The serum lipid, blood glucose, and HbAlc levels were within the normal range for all participants. No side effects were reported by the participants during the intervention. The participants in this study demonstrated a high compliance rate, with over 95% adhering to the prescribed macronutrient targets. This adherence was verified through dietary records and, for the HFKD group, ketone monitoring. Any deviations from the dietary protocols were promptly identified and rectified during counseling sessions, ensuring consistent adherence throughout the intervention period.
Table 1: Baseline characteristics of study population1
|
Characteristic |
HFKD | LFD |
| n | 14 |
14 |
|
Age, y |
26.2 5.6 | 26.9 7.0 |
| Body weight, kg | 76.9 8.5 |
73.1 6.7 |
|
High, cm |
158.6 2.6 | 157.5 4.2 |
| BMI, kg/m2 | 30.6 2.7 |
29.0 3.0 |
|
Waist circumference, cm |
88.6 9.8 | 84.4 7.6 |
| Subcutaneous fat, % | 44.9 7.3 |
43.5 7.0 |
|
Visceral fat, level |
12.7 | 11.6 4.6 |
| Total cholesterol, mmol/L | 187.6 32.1 |
169.2 21.2 |
|
Triglycerides, mmol/L |
71.1 35.0 | 85.9 38.1 |
| HDL cholesterol, mmol/L | 67.4 28.8 |
59.7 16.3 |
|
LDL cholesterol, mmol/L |
112.5 29.8 | 120.3 64.4 |
| Glucose, mmol/L | 98.6 9.2 |
89.4 11.1 |
|
HbA1c, % |
5.0 0.4 |
5.2 0.3 |
1Data are presented as mean (SD), unless otherwise indicated. BMI refers to body mass index (calculated as weight in kilograms divided by height in meters squared). HDL stands for high-density lipoprotein, and LDL stands for low-density lipoprotein.
Body composition
As presented in Table 2, both dietary interventions resulted in statistically significant reductions in body weight, BMI, and body fat. Body weight decreased from 76.9 ± 8.5 kg to 66.54 ± 7.7 kg in the HFKD group, representing a 13% reduction, and from 73.11 ± 6.7 kg to 65.4 ± 6.1 kg in the LFD group, representing a 10% reduction. BMI decreased by 13% in the HFKD group and by 9% in the LFD group; both changes were statistically significant (p < 0.001). Visceral fat level in HFKD group were dropped from 12.7 ± 4.9 to 9.6 ± 4.0, representing a 24%, and subcutaneous fat % decreased by 10% in the HFKD group; these changes were statistically significant (p < 0.001).
Table 2: Changes on body weight, BMI and body fat before and after the 12-weeks intervention2.
|
Parameter |
Before HFKD | After HFKD | P-value | % | Before LFD | After LFD | P-value | % |
|
Body weight (kg) |
76.9 ± 8.5 | 66.54 ± 7.7 | <0.001* | 13% | 73.11 ± 6.7 | 65.4 ± 6.1 | <0.001* | 10% |
|
BMI |
30.57 ± 2.7 | 26.50 ± 2.7 | <0.001* | 13% | 29.0 ± 3.0 | 26.2 ± 2.9 | <0.001* |
9% |
| Subcutaneous fat, % | 43.4 ± 7.0 | 38.9 ± 7.3 | <0.001* | 10% | 44.89 ± 7.3 | 39.0 ± 5.1 | <0.001* |
13% |
| Visceral Fat (level) | 12.7 ± 4.9 | 9.6 ± 4.0 | <0.001* | 24% | 11.6 ± 4.6 | 9.6 ± 4.2 | <0.001* |
17% |
2Body weight, BMI, and body fat of participants before and after following the high-fat ketogenic diet (HFKD) (n=14) and low-fat diet (LFD) (n=14). Values are presented as means ± SD. Data were analyzed using paired-samples t-test, with *p < 0.05 indicating statistical significance.
Cardiovascular diseases risk factors.
Our results indicate a decrease in total cholesterol levels with a statistically significant effect (P < 0.05) in the LFD group, showing a reduction of 9%. In contrast, the HFKD group experienced a 3% decrease in total cholesterol, which was not statistically significant (P > 0.05). For participants following the HFKD, there was a significant decrease in triglyceride levels by 25% (P = 0.029), whereas the LFD group showed a slight 6% increase in triglycerides with no significant difference (P > 0.05) at a 95% confidence level. Additionally, significant differences in LDL levels were observed: the LFD group had a significant 21% decrease (P < 0.05), while the HFKD group had a very slight, non-significant decrease of 1% (P > 0.05). As for HDL levels, both diets saw a decrease 4% for the HFKD and 15% for the LFD—with no significant differences before and after the participants followed the diets (Table 3). In the HFKD participants, there was a significant decrease in fasting glucose levels of 13% in this group (p = 0.006) after followed the diet for 12 weeks but no significant change in the LFD group (p > 0.05). However, there was a slight decrease in cumulative sugar of 0.9%, which was not statistically significant (p > 0.05) in the HFKD group. Regarding SBP, there was a statistically significant decrease of 7% in the HFKD group (p = 0.04). These results showed that, while both diets resulted in some changes, HFKD had more significant effects on triglyceride, glucose levels and SBP than LFD (Table 3).
Table 3: Impact of HFKD and LFD on Cardiovascular Risk Factors during the 12-Week Intervention3
|
Parameter |
Before HFKD | After HFKD | P-Value | % | Before LFD | After LFD | P-Value |
|
Total cholesterol (mg/dl) |
187.6 ± 32.1 | 180.7 ± 31.4 | 0.398 | 3% | 169.2 ± 21.2 | 153.0 ± 23.0 | 0.014* |
| Triglycerides (mg/dl) | 85.8 ± 38.1 | 64.3 ± 15.1 | 0.029* | 25% | 71.1 ± 35.0 | 75.6 ± 44.5 |
0.419 |
|
HDL (mg/dl) |
59.6 ± 16.3 | 57.1 ± 18.4 | 0.653 | 4% | 67.4 ± 28.8 | 56.6 ± 18.5 |
0.053 |
| LDL (mg/dl) | 112.5 ± 29.8 | 111.4 ± 24.9 | 0.870 | 1% | 120.3 ± 64.4 | 93.9 ± 45.7 |
0.030* |
|
HbAic (%) |
5.0 ± 0.4 | 4.9 ± 0.4 | 0.709 | 0.9% | 5.2 ± 0.3 | 5.2 ± 0.5 |
0.696 |
|
Glucose (mg/dl) |
98.6 ± 9.2 | 85.0 ± 9.0 | 0.006* | 13% | 89.4 ± 11.1 | 90.4 ± 10.6 | 0.522 |
| SBP (mm Hg) | 123.5 ± 11.8 | 114.7 ± 14.3 | 0.044* | 7% | 115.0± 15.5 | 113.9 ± 11.8 |
0.836 |
|
DBP (mm Hg) |
74.4 ± 7.5 | 74.7 ± 11.2 | 0.921 | 0.3% | 71.9± 9.7 | 67.1. ± 7.6 |
0.155 |
3Total cholesterol, triglycerides, HDL (high-density lipoprotein), LDL (low-density lipoprotein), HbA1c, glucose, SBP (systolic blood pressure), and DBP (diastolic blood pressure) of participants before and after following the high-fat ketogenic diet (HFKD) (n=14) and low-fat diet (LFD) (n=14). Values are presented as means ± SD. Data were analyzed using paired-samples t-test, with *p < 0.05 indicating statistical significance.
Discussion
In this intervention study, we tested the hypothesis that a high-fat ketogenic diet (HFKD) would be more effective for weight loss compared to a low-fat diet (LFD) in overweight and obese healthy women. Our finding found that significant weight loss and body mass reductions in both groups. Similarly, studies have observed comparable weight loss results between high-fat ketogenic diets (HFKD) and low-fat diets (LFD), primarily due to reduced calorie intake. 20,21 Research comparing the effects of different diets on liver fat percentage in obese adults also found similar weight loss across groups.22. Moreover, evidence suggests that HFKD and LFD are equally effective for weight loss, although some findings indicate that HFKD may lead to greater reductions in body weight.10,23 The difference in these results could be due to individual differences in response to diet, study duration, or calorie intake.
Our study also revealed improvements in blood lipid levels in both groups, total cholesterol and LDL levels significantly decreased in the LFD group, while triglyceride levels significantly decreased in the HFKD group. These findings support the importance of dietary fat type in cardiovascular health. 24,25 As previously mentioned, in our study, both diets limited saturated fat to less than 10% and primarily used olive oil, which is high in monounsaturated and polyunsaturated fatty acids and beneficial for cardiovascular health. 26,27 Elevated triglyceride levels are associated with high carbohydrate intake because excess carbohydrates can be converted to triglycerides.28 Furthermore, excess carbohydrates can be converted into triglycerides through a process called de novo lipogenesis.29 When carbohydrate intake exceeds the body’s immediate energy needs, the surplus is converted into fatty acids in the liver, which are then esterified to form triglycerides. 30 These triglycerides are transported to adipose tissue for storage. 28 A recent study reported that participants who followed a high-carbohydrate diet had higher triglyceride levels than those on a low-carbohydrate diet.31 Moreover, recent studies suggested that carbohydrate reduction and restriction can help lower triglyceride levels and improve overall lipid profiles and cardiovascular health. 32,33
This study showed decreases in total cholesterol and LDL levels in the LFD group, which is consistent with previous research.24 No significant difference in LDL levels was observed in the HFKD group, which is in line with previous studies that observed weight loss but increased LDL levels with HFKD. 23,34,35 Previous studies have investigated the effects of LFD on lipid profiles and found a significant reduction in LDL cholesterol levels, possibly due to reduced saturated fat and cholesterol intake.36, A 12-month randomized trial revealed that a low-fat diet (LFD) significantly reduced LDL cholesterol compared to a low-carbohydrate diet.34 This finding aligns with our findings and suggests that reducing dietary fat intake can lead to favorable changes in LDL levels. Furthermore, our results indicated that HFKD contributed to a statistically significant reduction in blood glucose levels, which aligns with studies that found a significant reduction in the blood glucose levels of participants following low-carb diets.21,38,39,40 One of the mechanisms of decreased level of blood glucose is induces a state of ketosis in which the body relies on fat for energy instead of carbohydrates, leading to various metabolic adaptations. 8 HFKD involves limited carbohydrate consumption (10% of total energy intake in this study), which directly reduces blood glucose levels. Moreover, the metabolic state of ketosis enhances fat oxidation and reduces glucose utilization, which leads to lower insulin levels. 41,42
Conclusion
To the best of our knowledge, this trial is the first controlled intervention study to directly compare the effects of a high-fat ketogenic diet (HFKD) and a low-fat diet (LFD) on overweight and obese women in Saudi Arabia. Our findings demonstrate that HFKD and LFD both led to significant weight loss and improvements in CVD risk factors, with distinct benefits observed for each diet. HFKD was led to significant lower triglyceride levels, improvements in glycemic control and SBP and visceral fat reduction, emphasizing its potential for enhancing metabolic health. In contrast, LFD was particularly effective in lowering cholesterol levels, making it advantageous for individuals focusing on lipid profile management. These results underscore the importance of calorie restriction, dietary fat type, and individual variability in managing obesity and associated health risks. Future research should involve larger sample sizes that include both genders, with extended study durations, to explore the long-term effects of these dietary interventions on obesity treatment and weight loss. Additionally, further investigation into the mechanisms underlying the impact of HFKD and LFD on health outcomes is needed.
Acknowledgement
We would like to express our sincere gratitude to the participants for dedicating their time and effort to this study. Their commitment and contributions to the data collection process were invaluable. We also extend our heartfelt thanks to the nurses at the medical center at King Faisal University for their assistance and support throughout the study. Their collaboration and professionalism were essential in making this research possible.
Funding Sources
This work was supported by the Deanship of Scientific Research at King Faisal University, Saudi Arabia (grant number KFU242635).
Conflict of Interest
The author(s) do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
The study received approval from the King Faisal University Ethics Committee (KFU – REC – 2021 – OCT EA00089).
Informed Consent Statement.
Informed consent was obtained from all participants involved in the study.
Permission to reproduce material from other sources.
This statement does not apply to this article.
Clinical Trial Registration
The clinical trial was registered at ClinicalTrials.gov with the registration number (ID: NCT05811702).
Author Contributions
- Atheer Ahmad. Alnoubi: Data Collection, Methodology, Writing – Original Draft.
- Randah Miqbil. Alqurashi: Conceptualization, Methodology, Writing – Original Draft, Review, Editing, Supervision and Project Administration.
References
- Kumar K. The global obesity epidemic: current trends and future perspectives. Journal of Global Health. 2023; 13(1): 01004.
- World Health Organization. Obesity and Overweight (2024). Available online at: WHO (accessed June 20, 2024).
- World Health Organization. World Health Organization Diabetes Country Profiles, Saudi Arabia (2016). Available online at: WHO (accessed June 20, 2024).
- Pronk NP, Anderson LH, Crain AL, Martinson BC, O’Connor PJ, Sherwood NE, Whitebird RR, Fine LJ, Flum DR, Vollmer WM. The benefits of weight loss: a review of the evidence and implications for a population approach to weight management. Journal of Cardiopulmonary Rehabilitation and Prevention. 2022; 42(1): 21–29.
- Aaseth J, Ellefsen S, Alehagen U, Sundfør TM, Alexander J. Diets and drugs for weight loss and health in obesity–An update. Biomedicine & Pharmacotherapy. 2021; 140: 111789.
CrossRef - McGaugh J, Barthel S. The ketogenic diet’s rise in popularity: a 2020 trend analysis. Journal of Nutrition & Health Sciences. 2022; 9(1): 1081.
- O’Neill S, Raggi P. The ketogenic diet: pros and cons. Nutrition & Diabetes. 2020; 10(1): 3.
CrossRef - Sakr EH, Fayez R, Taha HS, Soliman AM, Ghanem N. Ketosis and its metabolic effects: from basics to clinical implications. Journal of Clinical Endocrinology & Metabolism. 2023; 108(3): 611–621.
- Elamin MB, Murad MH, Elamin KB, Haydour Q. The effects of low-carbohydrate ketogenic diets vs. low-fat diets on weight loss and cardiovascular risk factors: a meta-analysis of randomized controlled trials. Nutrition, Metabolism and Cardiovascular Diseases. 2020; 30(5): 744–755.
- Hu T, Mills KT, Yao L, Demanelis K, Eloustaz M, Yancy WS Jr., Kelly TN, He J, Bazzano LA. Effects of low-carbohydrate diets vs. low-fat diets on metabolic risk factors: a meta-analysis of randomized controlled clinical trials. American Journal of Epidemiology. 2012; 176(S7): S44–S54.
CrossRef - Ministry of Health. Ketogenic Diet for Epilepsy Treatment: Guidelines for Practitioners. Available online at: MOH (accessed June 20, 2024).
- FAO and WHO. Sustainable healthy diets – Guiding principles. 2019. Available online at: WHO (accessed June 20, 2024).
- Iacovides S, Cho LW, Patil R. Randomization and allocation concealment in clinical trials: a practical guide. BMJ Evidence-based Medicine. 2022; 27(4): 221–225.
- Mustafidah Z, Alwi Q, Purnamasari A. The role of diet and nutrition in the prevention of chronic diseases: a review. Nutrition & Food Science. 2020; 50(4): 649–656.
- dos Santos Quaresma MVL, Arruda SF, Carvalheira JBC. Effect of ketogenic and low-fat diets on body composition and inflammatory markers: a randomized controlled trial. European Journal of Clinical Nutrition. 2022; 76(3): 438–446.
- Roza AM, Shizgal HM. The Harris Benedict equation reevaluated: resting energy requirements and the body cell mass. American Journal of Clinical Nutrition. 1984; 40(1): 168–182.
CrossRef - McCance RA, Widdowson EM. McCance and Widdowson’s The Composition of Foods: Seventh Summary Edition. Royal Society of Chemistry, 2014.
- Urbain P, Bertz H. Monitoring ketosis: measurement methods and clinical application. International Journal of Clinical Practice. 2016; 70(3): 230–237.
- Brehm BJ, Seeley RJ, Daniels SR, D’Alessio DA. A randomized trial comparing a very low carbohydrate diet and a calorie-restricted low-fat diet on body weight and cardiovascular risk factors in healthy women. Journal of Clinical Endocrinology & Metabolism. 2003; 88(4): 1617–1623.
CrossRef - Jonasson JM, Clausen T, Lissner L, Sundh V, Björkelund C. Effects of a low-carbohydrate high-protein diet vs. a low-fat diet on weight loss and cardiovascular risk factors in obese women: a randomized controlled trial. European Journal of Clinical Nutrition. 2014; 68(2): 130–136.
- Petrisko Y, Palmer J, Komar S. Comparison of low-carb and low-fat diets: a meta-analysis. Nutrients. 2020; 12(10): 3007.
- Crabtree CD, Simpson AM, Magon N. Comparative study of ketogenic, low-fat, and moderate-carbohydrate diets on liver fat percentage in obese adults. Obesity Reviews. 2021; 22(11): e13250.
- Dong, T., Guo, M., Zhang, P., Sun, G., Chen, B. The effects of low-carbohydrate diets on cardiovascular risk factors: a meta-analysis. PloS one. 2020; 15(1), e0225348.
CrossRef - Schwingshackl L, Hoffmann G. Long-term effects of low-fat vs. high-fat diets on blood lipids and cardiovascular risk: a systematic review and meta-analysis. Journal of the Academy of Nutrition and Dietetics. 2013; 113(12): 1640-1661.
CrossRef - Ren J, Grundy SM, Liu J. Comparison of low-carbohydrate and low-fat diets on metabolic risk factors: a meta-analysis. Nutrients. 2018; 10(6): 768.
- Mehmood A, Naseer R, Arif M, Khan R. The role of monounsaturated and polyunsaturated fatty acids in cardiovascular health: a review. Journal of Cardiovascular Medicine. 2020; 21(6): 472-481.
- Tagliamonte S, Ferrara L, Marfella R. Olive oil consumption and cardiovascular risk: insights from epidemiological studies and randomized trials. Journal of Nutritional Biochemistry. 2023; 108, 109118.
- Yki-Järvinen, H., Luukkonen, P. K., Hodson, L., & Moore, J. B. Dietary carbohydrates and fats in nonalcoholic fatty liver disease. Nature reviews Gastroenterology & hepatology. 2021; 18(11), 770-786.
CrossRef - Song Z, Xiaoli AM, Yang F. Regulation and metabolic significance of de novo lipogenesis in adipose tissues. Nutrients. 2018; 10(10): 1383.
CrossRef - Hydes T, Alam U, Cuthbertson DJ. The impact of macronutrient intake on non-alcoholic fatty liver disease (NAFLD): too much fat, too much carbohydrate, or just too many calories? Frontiers in Nutrition. 2021; 8: 640557.
CrossRef - Wachsmuth NB, Aberer F, Haupt S, Schierbauer JR, Zimmer RT, Eckstein ML, Zunner B, Schmidt W, Niedrist T, Sourij H, Moser O. The impact of a high-carbohydrate/low-fat vs. low-carbohydrate diet on performance and body composition in physically active adults: a cross-over controlled trial. Nutrients. 2022; 14(3): 423.
CrossRef - Gram‐Kampmann, E. M., Hansen, C. D., Hugger, M. B., Jensen, J. M., Brønd, J. C., Hermann, A. P., Krag, A., Olsen, M. H., Beck-Nielsen, H., Højlund, K. Effects of a 6‐month, low‐carbohydrate diet on glycaemic control, body composition, and cardiovascular risk factors in patients with type 2 diabetes: An open‐label randomized controlled trial. Diabetes, Obesity and Metabolism. 2022; 24(4), 693-703.
CrossRef - Ebbeling CB, Feldman HA, Klein GL, Wong JMW, Bielak L, Steltz SK, Luoto PK, Wolfe RR, Wong WW, Ludwig DS. Effects of a low carbohydrate diet on energy expenditure during weight loss maintenance: randomized trial. BMJ. 2018; 363: k4583.
CrossRef - Gardner CD, Trepanowski JF, Del Gobbo LC, Hauser ME, Rigdon J, Ioannidis JPA, Desai M., King A C. Effect of low-fat vs. low-carbohydrate diet on 12-month weight loss in overweight adults and the association with genotype pattern or insulin secretion: the DIETFITS randomized clinical trial. JAMA. 2018; 319(7): 667-679.
CrossRef - Binobead M, Al-Mugheed K, Al Ali Y. Comparative effects of ketogenic and low-fat diets on weight loss and cardiovascular risk factors: a systematic review. Saudi Journal of Biological Sciences. 2023; 30(2): 1025-1033.
- Lei Y, Su SC, Cockerell J. Effects of low-fat vs. low-carbohydrate diets on LDL cholesterol levels: a randomized trial. Nutrition & Metabolism. 2022; 19(1): 33.
- Wachsmuth NB, Sprenger M, Simon P. Effects of a low-fat diet on lipid profiles in endurance athletes: a randomized controlled trial. Journal of the International Society of Sports Nutrition. 2022; 19(1): 18.
- Saslow LR, Jones LM, Sen A, Wolfson JA, Diez HL, O’Brien A, Leung C.W., Bayandorian H., Daubenmier J., Missel A L., Richardson C. Comparing very low-carbohydrate vs DASH diets for overweight or obese adults with hypertension and prediabetes or type 2 diabetes: a randomized trial. The Annals of Family Medicine. 2023; 21(3): 256-263.
CrossRef - Hyde, P. N., Sapper, T. N., Crabtree, C. D., LaFountain, R. A., Bowling, M. L., Buga, A., Fell, B., McSwiney, F. T., Dickerson, R.M., Miller, V.J., Scanding D,M., Simonetti, O, P., Phinney, S.D., Kraemer, W. J., King, S.A., Krauss, R.M., Volek, J.S. Dietary carbohydrate restriction improves metabolic syndrome independent of weight loss. JCI insight,2019; 4(12).
CrossRef - Han, Y., Cheng, B., Guo, Y., Wang, Q., Yang, N., & Lin, P. A low-carbohydrate diet realizes medication withdrawal: a possible opportunity for effective glycemic control. Frontiers in endocrinology, 2021; 12, 779636.
CrossRef - Sakr, H. F., Sirasanagandla, S. R., Das, S., Bima, A. I., & Elsamanoudy, A. Z. Low-carbohydrate ketogenic diet for improvement of glycemic control: Mechanism of action of ketosis and beneficial effects. Current Diabetes Reviews. 2023; 19(2), 82-93.
CrossRef - Napoleão, A., Fernandes, L., Miranda, C., & Marum, A. P. Effects of calorie restriction on health span and insulin resistance: Classic calorie restriction diet vs. ketosis-inducing diet. Nutrients. 2021; 13(4), 1302.
CrossRef

This work is licensed under a Creative Commons Attribution 4.0 International License.







